

CD4 Donor Lymphocyte Infusion Can Cause Conversion of Chimerism Without GVHD by Inducing Immune Responses Targeting Minor Histocompatibility Antigens in HLA Class II
- PMID: 30619360
- PMCID: PMC6305328
- DOI: 10.3389/fimmu.2018.03016
CD4 Donor Lymphocyte Infusion Can Cause Conversion of Chimerism Without GVHD by Inducing Immune Responses Targeting Minor Histocompatibility Antigens in HLA Class II
Abstract
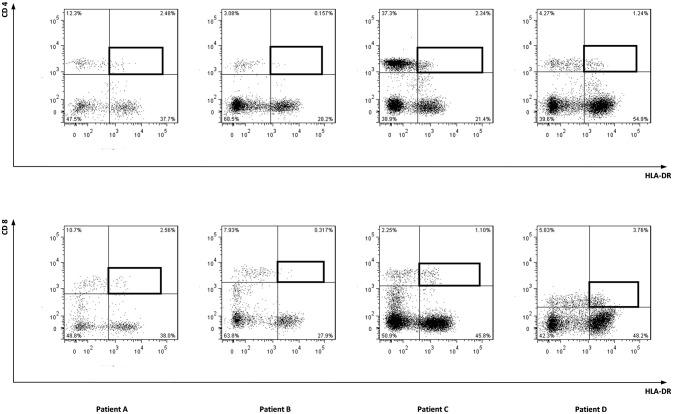
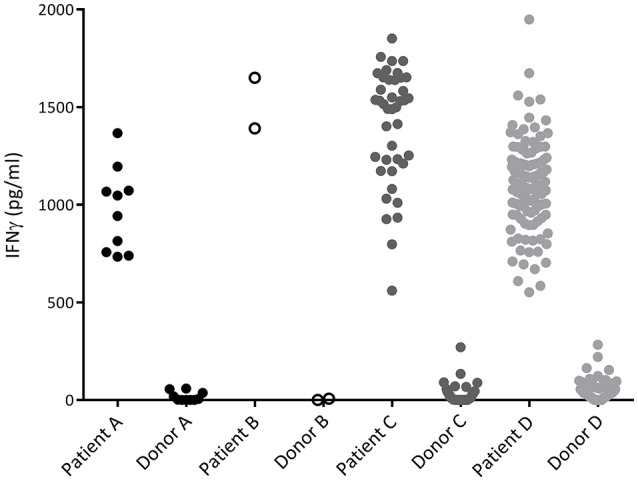
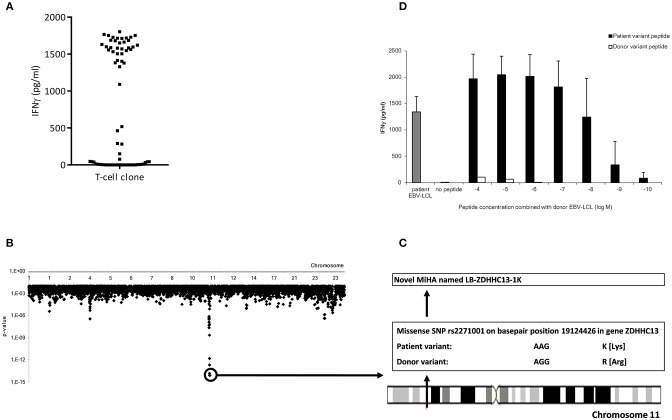
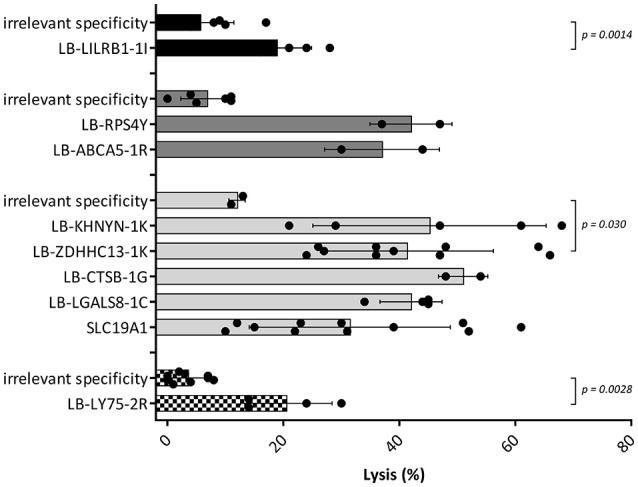
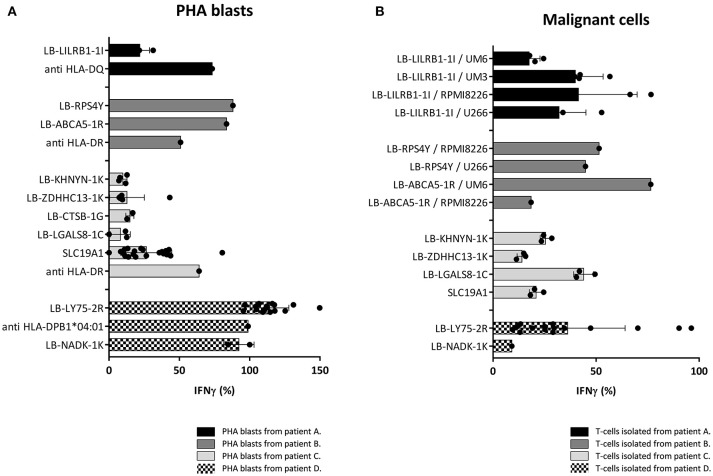
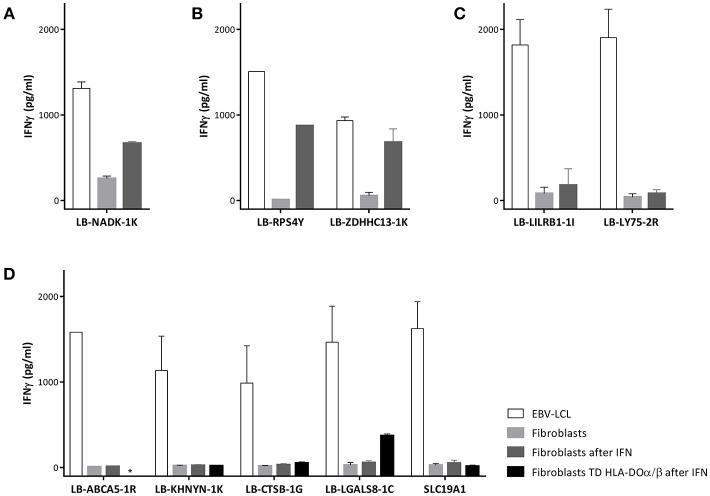
Under non-inflammatory conditions HLA class II is predominantly expressed on hematopoietic cells. Therefore, donor CD4 T-cells after allogeneic stem cell transplantation (alloSCT) may mediate graft-vs.-leukemia reactivity without graft-vs.-host disease (GVHD). We analyzed immune responses in four patients converting from mixed to full donor chimerism without developing GVHD upon purified CD4 donor lymphocyte infusion (DLI) from their HLA-identical sibling donor after T-cell depleted alloSCT. In vivo activated T-cells were clonally isolated after CD4 DLI. Of the alloreactive T-cell clones, 96% were CD4 positive, illustrating the dominant role of CD4 T-cells in the immune responses. We identified 9 minor histocompatibility antigens (MiHA) as targets for alloreactivity, of which 8 were novel HLA class II restricted MiHA. In all patients, MiHA specific CD4 T-cells were found that were capable to lyse hematopoietic cells and to recognize normal and malignant cells. No GVHD was induced in these patients. Skin fibroblasts forced to express HLA class II, were recognized by only two MiHA specific CD4 T-cell clones. Of the 7 clones that failed to recognize fibroblasts, two targeted MiHA were encoded by genes not expressed in fibroblasts, presentation of one MiHA was dependent on HLA-DO, which is absent in fibroblasts, and T-cells recognizing the remaining 4 MiHA had an avidity that was apparently too low to recognize fibroblasts, despite clear recognition of hematopoietic cells. In conclusion, purified CD4 DLI from HLA-identical sibling donors can induce conversion from mixed to full donor chimerism with graft-vs.-malignancy reactivity, but without GVHD, by targeting HLA class II restricted MiHA.
Keywords: CD4 donor lymphocyte infusion; HLA class II; allogeneic stem cell transplantation; graft-vs.-tumor reactivity; minor histocompatibility antigen.
Figures
Similar articles
-
Identification of 4 new HLA-DR-restricted minor histocompatibility antigens as hematopoietic targets in antitumor immunity.Blood. 2009 Oct 22;114(17):3684-92. doi: 10.1182/blood-2009-03-208017. Epub 2009 Aug 25. Blood. 2009. PMID: 19706888
-
Collateral damage of nonhematopoietic tissue by hematopoiesis-specific T cells results in graft-versus-host disease during an ongoing profound graft-versus-leukemia reaction.Biol Blood Marrow Transplant. 2014 Jun;20(6):760-9. doi: 10.1016/j.bbmt.2014.03.002. Epub 2014 Mar 7. Biol Blood Marrow Transplant. 2014. PMID: 24607556
-
HLA class II upregulation during viral infection leads to HLA-DP-directed graft-versus-host disease after CD4+ donor lymphocyte infusion.Blood. 2013 Sep 12;122(11):1963-73. doi: 10.1182/blood-2012-12-470872. Epub 2013 Jun 18. Blood. 2013. PMID: 23777765 Clinical Trial.
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
-
Minor histocompatibility antigens to predict, monitor or manipulate GvL and GvHD after allogeneic hematopoietic cell transplantation.Best Pract Res Clin Haematol. 2024 Jun;37(2):101555. doi: 10.1016/j.beha.2024.101555. Epub 2024 May 15. Best Pract Res Clin Haematol. 2024. PMID: 39098803 Review.
Cited by
-
Beyond αβ T cells: NK, iNKT, and γδT cell biology in leukemic patients and potential for off-the-shelf adoptive cell therapies for AML.Front Immunol. 2023 Aug 15;14:1202950. doi: 10.3389/fimmu.2023.1202950. eCollection 2023. Front Immunol. 2023. PMID: 37654497 Free PMC article. Review.
-
HLA-DPB1 Reactive T Cell Receptors for Adoptive Immunotherapy in Allogeneic Stem Cell Transplantation.Cells. 2020 May 20;9(5):1264. doi: 10.3390/cells9051264. Cells. 2020. PMID: 32443793 Free PMC article.
-
Relapse after allogeneic hematopoietic stem cell transplantation in acute myeloid leukemia: an overview of prevention and treatment.Int J Hematol. 2022 Sep;116(3):330-340. doi: 10.1007/s12185-022-03416-7. Epub 2022 Jul 16. Int J Hematol. 2022. PMID: 35841458 Review.
-
Mutated DNMT3A creates a public HLADQ- binding neoantigen on acute myeloid leukemia.Front Immunol. 2025 Mar 13;16:1556121. doi: 10.3389/fimmu.2025.1556121. eCollection 2025. Front Immunol. 2025. PMID: 40151616 Free PMC article.
-
Development of TCR-T cell therapy targeting mismatched HLA-DPB1 for relapsed leukemia after allogeneic transplantation.Int J Hematol. 2023 Aug;118(2):252-266. doi: 10.1007/s12185-023-03621-y. Epub 2023 Jun 13. Int J Hematol. 2023. PMID: 37310580
References
-
- Pasquini MC, Devine S, Mendizabal A, Baden LR, Wingard JR, Lazarus HM, et al. . Comparative outcomes of donor graft CD34+ selection and immune suppressive therapy as graft-versus-host disease prophylaxis for patients with acute myeloid leukemia in complete remission undergoing HLA-matched sibling allogeneic hematopoietic cell transplantation. J Clin Oncol. (2012) 30:3194–201. 10.1200/JCO.2012.41.7071 - DOI - PMC - PubMed
-
- Kottaridis PD, Milligan DW, Chopra R, Chakraverty RK, Chakrabarti S, Robinson S, et al. . In vivo CAMPATH-1H prevents graft-versus-host disease following nonmyeloablative stem cell transplantation. Blood (2000) 96:2419–25. - PubMed
-
- Chakrabarti S, Mackinnon S, Chopra R, Kottaridis PD, Peggs K, O'Gorman P, et al. . High incidence of cytomegalovirus infection after nonmyeloablative stem cell transplantation: potential role of Campath-1H in delaying immune reconstitution. Blood (2002) 99:4357–63. 10.1182/blood.V99.12.4357 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials