

Four Months of a School-Based Exercise Program Improved Aerobic Fitness and Clinical Outcomes in a Low-SES Population of Normal Weight and Overweight/Obese Children With Asthma
- PMID: 30619785
- PMCID: PMC6297379
- DOI: 10.3389/fped.2018.00380
Four Months of a School-Based Exercise Program Improved Aerobic Fitness and Clinical Outcomes in a Low-SES Population of Normal Weight and Overweight/Obese Children With Asthma
Abstract
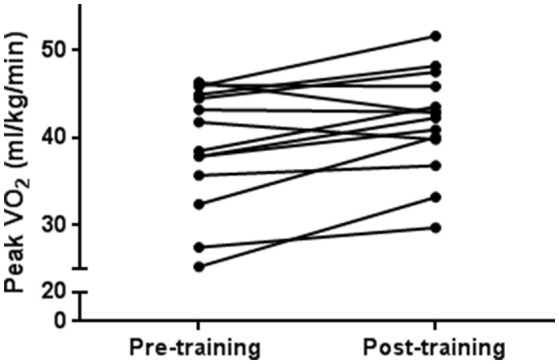
Introduction: Fitness can improve asthma management. However, children from disadvantaged and minority communities generally engage less in physical activity, and have increased obesity and asthma disease burden. The goal of this pilot study is to evaluate (1) the feasibility of an exercise intervention program in a school-based setting (attendance and fitness improvement) and (2) the effect of the intervention on fitness, asthma, and clinical outcomes in normal weight and overweight/obese children with asthma from low-SES population. Materials and Methods: Nineteen children, ages 6-13 years, from two elementary schools in Santa Ana, CA, a population with high percentage of Hispanic and low socioeconomic status, participated. Training sessions occurred at the schools during afterschool hours (3 sessions weekly × 4 months) and included mainly aerobic age-appropriate activities/games and a small component of muscle strength. Before and after the intervention, evaluations included pulmonary function testing, cardiopulmonary exercise testing (peak O2), assessments of habitual physical activity, body composition (DXA), asthma questionnaires, and blood (cardiometabolic risk factors). Results: Seventeen of 19 participants completed the study. Adherence to the program was 85%. Based on BMI %ile, 11 of the participants were overweight/obese and 8 were normal weight. Ten participants had persistent asthma and 9 children had intermittent asthma. Training was effective as peak O2 improved significantly (8.1%, SD ± 10.1). There was no significant change in BMI %ile but a significant improvement in lean body mass (1%, SD ± 2.0) and decrease in body fat (1.9%, SD ± 4.6). Asthma quality of life outcomes improved following the intervention in symptoms, emotional function, and overall. There was no change in asthma control or pulmonary function. Five of 10 participants with persistent asthma decreased their maintenance medications. Lipid levels did not change except HDL levels increased (46.1 ± 8.4 mg/dL to 49.5 ± 10.4 mg/dL, p = 0.04). Discussion: A school-based exercise intervention program designed specifically for children with asthma for a predominantly economically disadvantaged and minority population was feasible with good adherence to the program and substantial engagement from the schools, families and participants. The exercise intervention was effective with improvement in aerobic fitness, body composition, asthma quality of life, and lipid outcomes, setting the stage for a larger multicenter trial designed to study exercise as an adjunct medicine in children with asthma.
Keywords: aerobic fitness; asthma; low SES; obesity; school.
Figures
References
-
- Asthma Control Program N Asthma Facts: CDC's National Asthma Control Program Grantees. Centers Dis Control Prev (2013). Available online at: https://www.cdc.gov/asthma/pdfs/asthma_facts_program_grantees.pdf (Accessed March 6, 2017).