

Procalcitonin-Guided Antibiotic Therapy Reduces Antibiotic Use for Lower Respiratory Tract Infections in a United States Medical Center: Results of a Clinical Trial
- PMID: 30619913
- PMCID: PMC6306569
- DOI: 10.1093/ofid/ofy327
Procalcitonin-Guided Antibiotic Therapy Reduces Antibiotic Use for Lower Respiratory Tract Infections in a United States Medical Center: Results of a Clinical Trial
Abstract
Background: European trials using procalcitonin (PCT)-guided antibiotic therapy for patients with lower respiratory tract infections (LRTIs) have demonstrated significant reductions in antibiotic use without increasing adverse outcomes. Few studies have examined PCT for LRTIs in the United States.
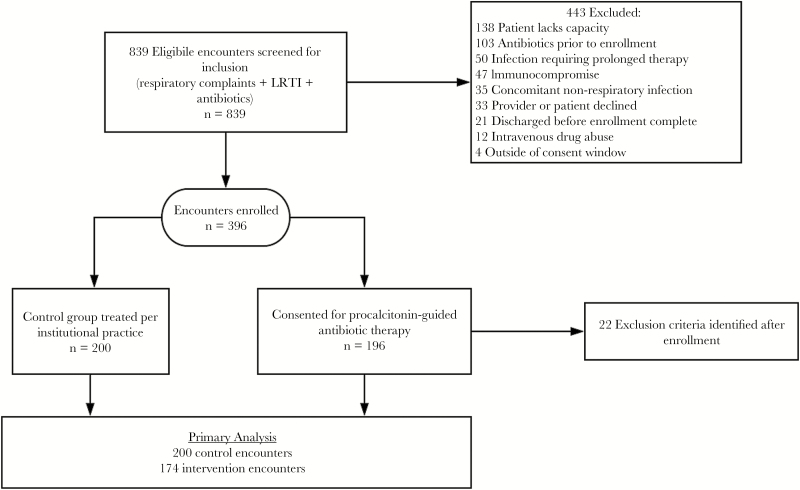
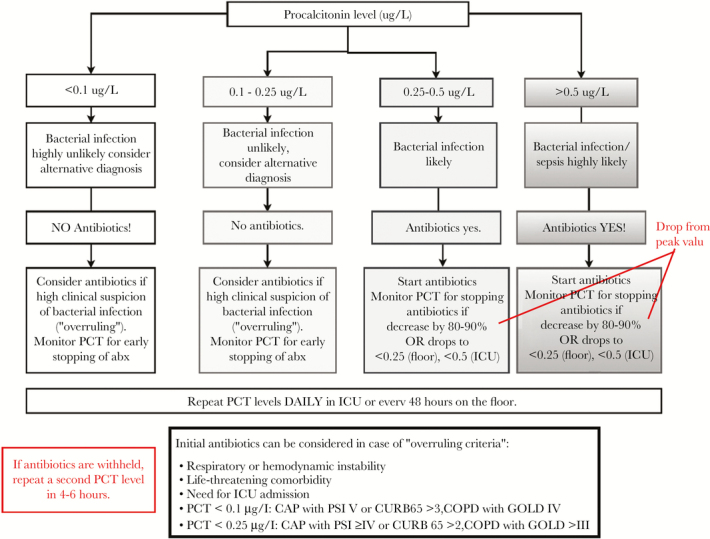
Methods: In this study, we evaluated whether a PCT algorithm would reduce antibiotic exposure in patients with LRTI in a US hospital. We conducted a controlled pre-post trial comparing an intervention group of PCT-guided antibiotic therapy to a control group of usual care. Consecutive patients admitted to medicine services and receiving antibiotics for LRTI were enrolled in the intervention. Providers were encouraged to discontinue antibiotics according to a PCT algorithm. Control patients were similar patients admitted before the intervention.
Results: The primary endpoint was median antibiotic duration. Overall adverse outcomes at 30 days comprised death, transfer to an intensive care unit, antibiotic side effects, Clostridium difficile infection, disease-specific complications, and post-discharge antibiotic prescription for LRTI. One hundred seventy-four intervention patients and 200 controls were enrolled. Providers complied with the PCT algorithm in 75% of encounters. Procalcitonin-guided therapy reduced median antibiotic duration for pneumonia from 7 days to 6 (P = .045) and acute exacerbation of chronic obstructive pulmonary disease (AECOPD) from 4 days to 3 (P = .01). There was no difference in the rate of adverse outcomes in the PCT and control groups.
Conclusions: A PCT-guided algorithm safely reduced the duration of antibiotics for treating LRTI. Utilization of a PCT algorithm may aid antibiotic stewardship efforts.This clinical trial was a single-center, controlled, pre-post study of PCT-guided antibiotic therapy for LRTI. The intervention (incorporation of PCT-guided algorithms) started on April 1, 2017: the preintervention (control group) comprised patients admitted from November 1, 2016 to April 16, 2017, and the postintervention group comprised patients admitted from April 17, 2017 to November 29, 2017 (Supplementary Figure 1). The study comprised patients admitted to the internal medicine services to a medical ward, the Medical Intensive Care Unit (MICU), the Cardiac Intensive Care Unit (CICU), or the Progressive Care Unit (PCU) "step down unit". The registration data for the trails are in the ClinicalTrials.gov database, number NCT0310910.
Keywords: antibiotic stewardship; clinical trials; lower respiratory tract infections; procalcitonin.
Figures

References
-
- Hecker MT, Aron DC, Patel NP, et al. . Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity. Arch Intern Med 2003; 163:972–8. - PubMed
-
- Szymczak J. Influencing antibiotic prescribing behavior: inpatient settings. In: Presidential Advisory Council on Combating Antibiotic Resistance. Washington, DC: 2017. HHS.gov. https://www.hhs.gov/sites/default/files/szymczak-91317.pdf.
-
- Claessens YE, Debray MP, Tubach F, et al. . Early chest computed tomography scan to assist diagnosis and guide treatment decision for suspected community-acquired pneumonia. Am J Respir Crit Care Med 2015; 192:974–82. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
