

Low hepatitis C prevalence in Belgium: implications for treatment reimbursement and scale up
- PMID: 30621662
- PMCID: PMC6325873
- DOI: 10.1186/s12889-018-6347-z
Low hepatitis C prevalence in Belgium: implications for treatment reimbursement and scale up
Abstract
Background: Prevalence data of chronic hepatitis C virus (HCV) infection are needed to estimate the budgetary impact of reimbursement of direct-acting antivirals (DAAs). In Belgium, the restricted reimbursement criteria are mainly guided by regional seroprevalence estimates of 0.87% from 1993 to 1994. In this first Belgian nationwide HCV prevalence study, we set out to update the seroprevalence and prevalence of chronic HCV infection estimates in the Belgian general population in order to guide decisions on DAA reimbursement.
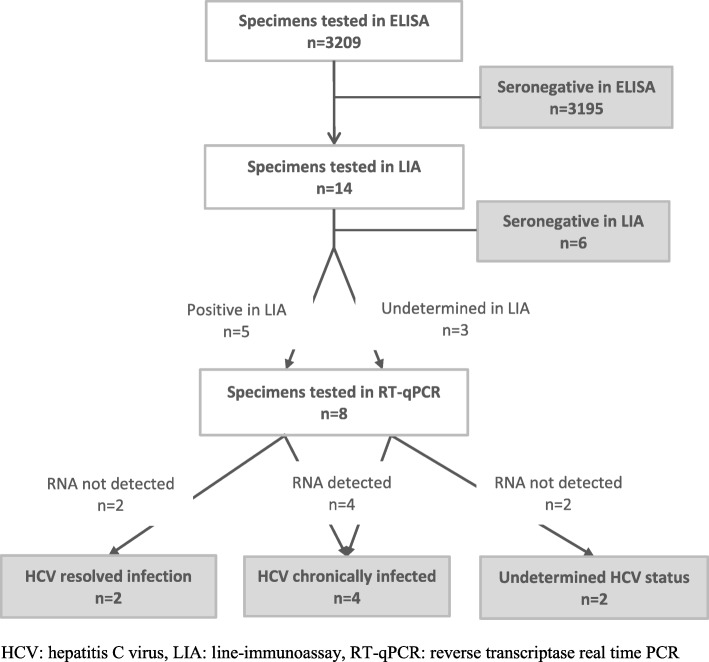
Methods: Residual sera were collected through clinical laboratories. We collected data on age, sex and district. HCV antibody status was determined with ELISA and confirmed with a line-immunoassay (LIA). In specimens with undetermined or positive LIA result, HCV viral load was measured. Specimens were classified seronegative, seropositive with resolved infection, indicative of chronic infection and with undetermined HCV status according to the test outcomes. Results were standardized for age, sex and population per district, and adjusted for clustered sampling.
Results: In total 3209 specimens, collected by 28 laboratories, were tested. HCV seropositivity in the Belgian general population was estimated to be 0.22% (95% CI: 0.09-0.54%), and prevalence of chronic HCV infection 0.12% (95% CI: 0.03-0.41). In individuals of 20 years and older, these estimates were 0.26% (95% CI: 0.10-0.64%) and 0.13% (95% CI: 0.04-0.43), respectively. Of the total estimated number of HCV seropositive individuals in Belgium, 66% were between 50 and 69 years old.
Conclusions: Prevalence of HCV seropositivity and chronic infection in the Belgian general population were low and comparable to many surrounding countries. These adjusted prevalences can help estimate the cost of reimbursement of DAAs and invite Belgian policy makers to accelerate the scaling up of reimbursement, giving all chronically infected HCV patients a more timely access to treatment.
Keywords: Belgium; Chronic hepatitis C virus infection; Direct-acting antivirals; Hepatitis C; Prevalence; Seroprevalence.
Conflict of interest statement
Ethics approval and consent to participate
The protocol was approved by the Ethics committee of the Antwerp University Hospital and the University of Antwerp (Registration number B300201316922) and the study was reported to the Commission for the Protection of Privacy. Since data were provided unlinked anonymous and residual blood specimens were used, an informed consent was not applicable. A waiver of informed consent was approved by the Ethics committee.
Consent for publication
Not applicable.
Competing interests
TV is a recipient of a 2014 mandate from the Belgian Foundation Against Cancer (mandate number: 2014–087) and previously received research funding from Gilead Sciences, Bristol-Myers-Squib and Roche Diagnostics. All other authors declared no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Hepatitis C: only a step away from elimination? Lancet. 2015;385(9973):1045. - PubMed
-
- Razavi H, Robbins S, Zeuzem S, Negro F, Buto M, Duberg A, et al. Hepatitis C virus prevalence and level of intervention required to achieve the WHO targets for elimination in the European Union by 2030: a modelling study. Lancet Gastroenterol Hepatol. 2017;2(5):325–336. doi: 10.1016/S2468-1253(17)30045-6. - DOI - PubMed
-
- World Health Organization (WHO). Hepatitis C Fact sheet. Geneva: WHO. http://www.who.int/mediacentre/factsheets/fs164/en/. Accessed 12 Sept 2018.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
