

Non-inferiority of dose reduction versus standard dosing of TNF-inhibitors in axial spondyloarthritis
- PMID: 30621746
- PMCID: PMC6323809
- DOI: 10.1186/s13075-018-1772-z
Non-inferiority of dose reduction versus standard dosing of TNF-inhibitors in axial spondyloarthritis
Abstract
Objective: The objective was to determine if dose reduction is non-inferior to full-dose TNFi to maintain low disease activity (LDA) in patients already in remission with TNFi, in axial spondyloarthritis.
Methods: Randomized, parallel, non-inferiority, open-label multicentre clinical trial. Patients were eligible if they had axial spondyloarthritis and had been in clinical remission for ≥ 6 months with any available TNFi (adalimumab, etanercept, infliximab, golimumab) at the dose recommended by product labelling. Patients were randomized by automated central allocation to continue the same TNFi dose schedule, or to reduce the dose by roughly half according to the protocol. The main outcome was the proportion of subjects with LDA after 1 year. Serious adverse reactions or infections were recorded.
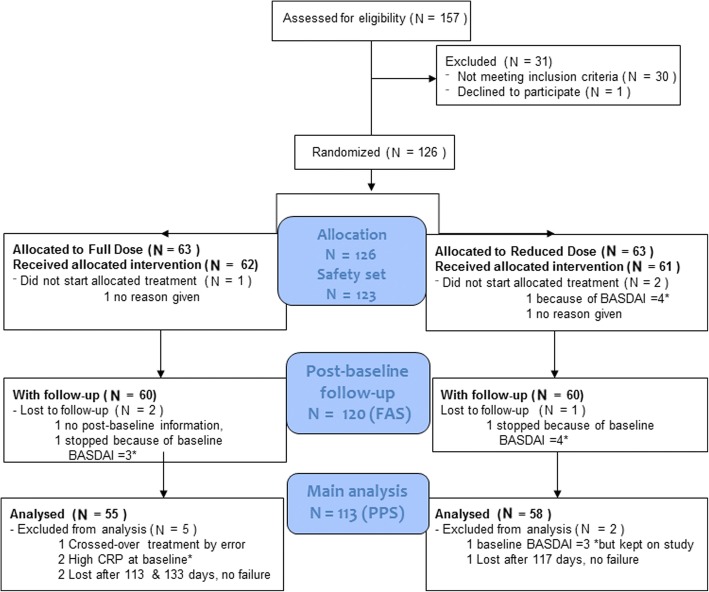
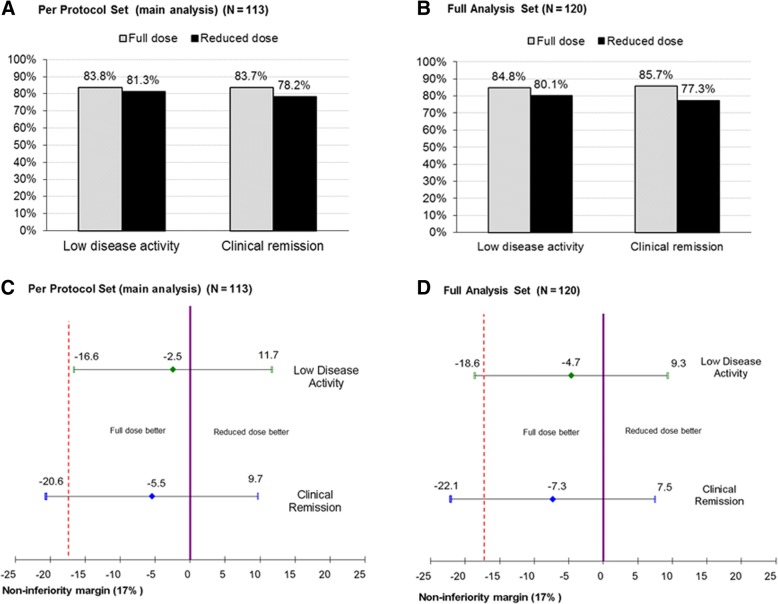
Results: The trial stopped due to end of the funding period, after 126 patients were randomized; 113 patients (84.1% male, mean age (SD) 45.6 (13.0) years) were included in the main per-protocol subset. Non-inferiority was concluded for LDA at 1 year (47/55 (83.8%) patients in the full-dose and 48/58 (81.3%) patients in the reduced-dose arm, adjusted difference (95% CI) - 2.5% (- 16.6% to 11.7%)). Serious adverse reactions or infections were reported in 7/62 patients (11.3%) assigned to full dose and 2/61 patients (3.3%) assigned to reduced dose (p value = 0.164).
Conclusion: In patients with ankylosing spondylitis in clinical remission for at least 6 months, dose reduction is non-inferior to full TNF inhibitor doses to maintain LDA after 1 year. Serious adverse events may be less frequent with reduced doses.
Trial registration: EU Clinical Trials Registry, EudraCT 2011-005871-18 and ClinicalTrials.gov, NCT01604629 .
Keywords: Dose-tapering; Non-inferiority; Spondyloarthritis; TNF inhibitors.
Conflict of interest statement
Ethics approval and consent to participate
The trial was performed according to the study protocol and protocol amendments, which were approved by the Ethics Committee for Clinical Research of the participating sites and by the Spanish Agency for Medicines and Health Products, and complied with the ethical principles of biomedical research, Good Clinical Practice [35] and applicable Spanish legislation. Two amendments to the protocol reflected in the clinical trial registration sites were implemented after recruitment was initiated, which referred to inclusion of new investigators and recruiting sites, and to allow collection of blood samples for measurement of inflammatory mediators, drug plasma measurements and ADA.
Consent for publication
All authors have read and approved the final version and consent to publication.
Competing interests
No author has received any private funding, nor has any been influenced in the preparation of the manuscript. The following authors declare that they have no competing interests: CP, FT, CAS, AV and GC. In the past 2 years, JG has received grants to attend congresses and educational courses, has obtained fees for scientific consultancies and has received speaking fees and fees for participation in educational programmes from the following companies: Roche, MSD, Pfizer, AbbVie, Janssen Cilag, UCB Pharma, Novartis and Celgene. EdM has received grant/research support from AbbVie and Pfizer, honorarium as a speaker from Abbvie, MSD and Novartis and consultant fees from Abbvie and Novartis. JS has obtained grants to attend congresses, speaking fees and fees for participation in educational programmes from Abbvie, Pfizer, MSD, Roche, UCB and Menarini. XJ has attended advisory board meetings of Celgene, has received investigational grants from Abbvie and Pfizer and has received fees for participation in educational programmes from MSD, Pfizer and Abbvie. RS has received speaking fees and fees for attending advisory boards from Abbott/Abbvie, Bristol-Myers Squibb, MSD, Roche, UCB and Pfizer, investigational grants from Bristol-Myers Squibb, MSD, Roche, UCB, Pfizer, FER and SCR and funding for educational projects from MSD, Bristol-Myers Squibb and Abbvie.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Tapering bDMARDs in axial SpA - what is the current evidence?Nat Rev Rheumatol. 2019 Jun;15(6):322-324. doi: 10.1038/s41584-019-0201-2. Nat Rev Rheumatol. 2019. PMID: 30903025 No abstract available.
Similar articles
-
Dose reduction and withdrawal strategy for TNF-inhibitors in psoriatic arthritis and axial spondyloarthritis: design of a pragmatic open-label, randomised, non-inferiority trial.Trials. 2020 Jan 15;21(1):90. doi: 10.1186/s13063-019-4000-5. Trials. 2020. PMID: 31941544 Free PMC article. Clinical Trial.
-
Effects of tapering tumor necrosis factor inhibitor on the achievement of inactive disease in patients with axial spondyloarthritis: a nationwide cohort study.Arthritis Res Ther. 2019 Jul 4;21(1):163. doi: 10.1186/s13075-019-1943-6. Arthritis Res Ther. 2019. PMID: 31272498 Free PMC article.
-
Comparison of drug survival on adalimumab, etanercept, golimumab and infliximab in patients with axial spondyloarthritis.PLoS One. 2019 May 30;14(5):e0216746. doi: 10.1371/journal.pone.0216746. eCollection 2019. PLoS One. 2019. PMID: 31145730 Free PMC article.
-
Risk of disease flare in spondyloarthritis patients after tapering tumor necrosis factor inhibitors: A meta-analysis and literature review.Int Immunopharmacol. 2024 Jun 15;134:112167. doi: 10.1016/j.intimp.2024.112167. Epub 2024 May 15. Int Immunopharmacol. 2024. PMID: 38754279
-
Biologic therapies in the spondyloarthritis: new opportunities, new challenges.Curr Opin Rheumatol. 2003 Jul;15(4):394-407. doi: 10.1097/00002281-200307000-00005. Curr Opin Rheumatol. 2003. PMID: 12819466 Review.
Cited by
-
Biologic Abatement and Capturing Kids' Outcomes and Flare Frequency in Juvenile Spondyloarthritis (BACK-OFF JSpA): study protocol for a randomized pragmatic trial.Trials. 2023 Feb 8;24(1):100. doi: 10.1186/s13063-022-07038-6. Trials. 2023. PMID: 36755328 Free PMC article.
-
De-Escalation of Anti-Tumor Necrosis Factor Alpha Agents and Reduction in Adverse Effects: A Systematic Review.Biomedicines. 2022 Apr 29;10(5):1034. doi: 10.3390/biomedicines10051034. Biomedicines. 2022. PMID: 35625771 Free PMC article. Review.
-
Association between cumulative TNF inhibitor dose and spinal radiographic progression in radiographic axial spondyloarthritis in patients with modified stoke ankylosing spondylitis spinal score ⩽24.Ther Adv Musculoskelet Dis. 2025 Jul 27;17:1759720X251358022. doi: 10.1177/1759720X251358022. eCollection 2025. Ther Adv Musculoskelet Dis. 2025. PMID: 40734687 Free PMC article.
-
Dosage reduction and discontinuation of biological disease-modifying antirheumatic drugs in patients with rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis: protocol for a pragmatic, randomised controlled trial (the BIOlogical Dose OPTimisation (BIODOPT) trial).BMJ Open. 2019 Jul 9;9(7):e028517. doi: 10.1136/bmjopen-2018-028517. BMJ Open. 2019. PMID: 31292181 Free PMC article.
-
Impact of tapering targeted therapies (bDMARDs or JAKis) on the risk of serious infections and adverse events of special interest in patients with rheumatoid arthritis or spondyloarthritis: a systematic analysis of the literature and meta-analysis.Arthritis Res Ther. 2020 Apr 29;22(1):97. doi: 10.1186/s13075-020-02188-x. Arthritis Res Ther. 2020. PMID: 32349791 Free PMC article.
References
-
- Braun J, Pincus T. Mortality, course of disease and prognosis of patients with ankylosing spondylitis. Clin Exp Rheumatol. 2002;20(6 Suppl 28):S16–S22. - PubMed
-
- Smolen JS, Braun J, Dougados M, Emery P, Fitzgerald O, Helliwell P, Kavanaugh A, Kvien TK, Landewe R, Luger T, et al. Treating spondyloarthritis, including ankylosing spondylitis and psoriatic arthritis, to target: recommendations of an international task force. Ann Rheum Dis. 2014;73(1):6–16. doi: 10.1136/annrheumdis-2013-203419. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
