

Transcriptomic Profiling of the Tumor Microenvironment Reveals Distinct Subgroups of Clear Cell Renal Cell Cancer: Data from a Randomized Phase III Trial
- PMID: 30622105
- PMCID: PMC6697163
- DOI: 10.1158/2159-8290.CD-18-0957
Transcriptomic Profiling of the Tumor Microenvironment Reveals Distinct Subgroups of Clear Cell Renal Cell Cancer: Data from a Randomized Phase III Trial
Abstract
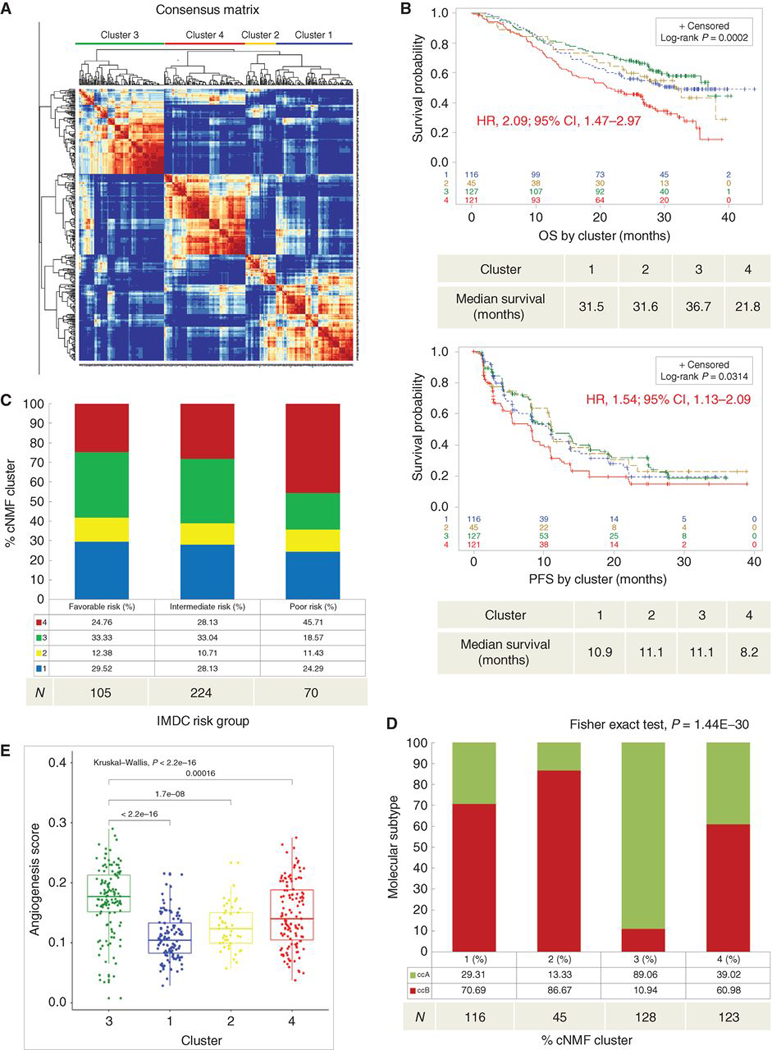
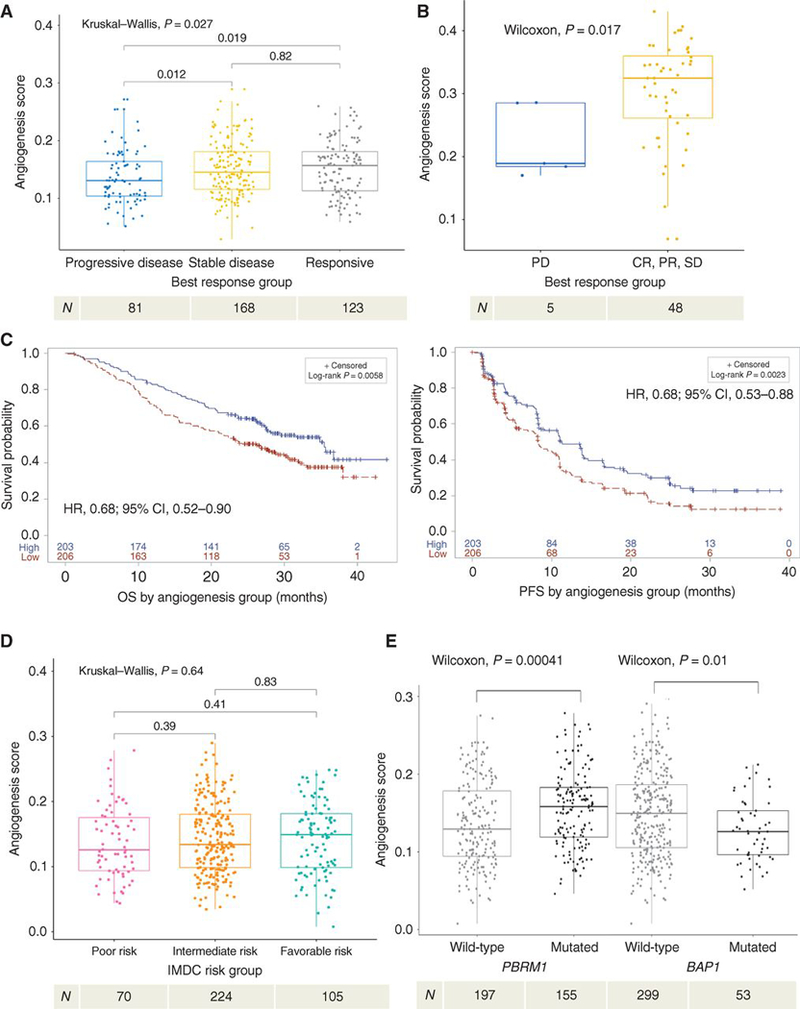
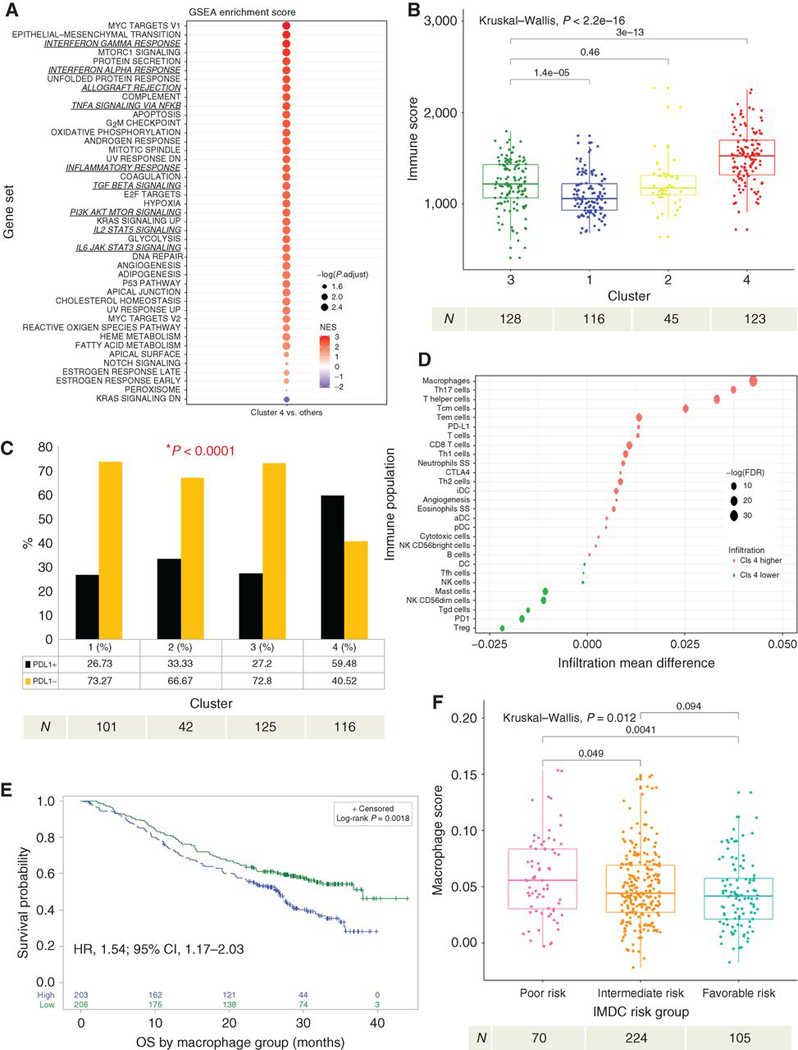
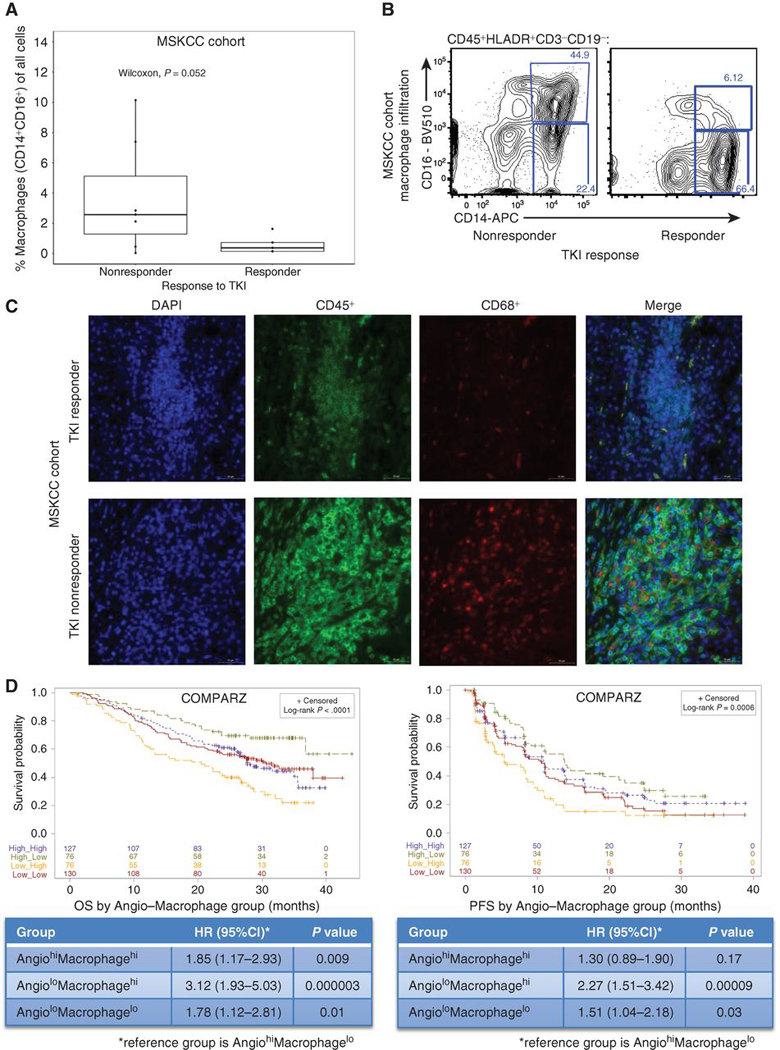
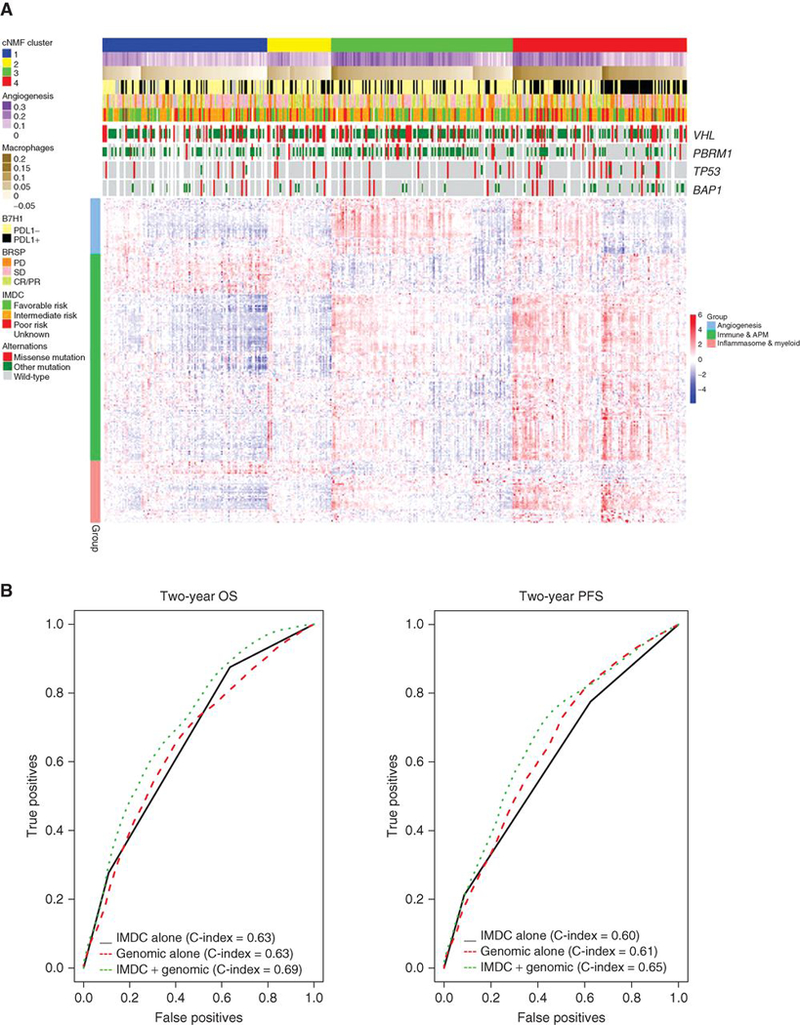
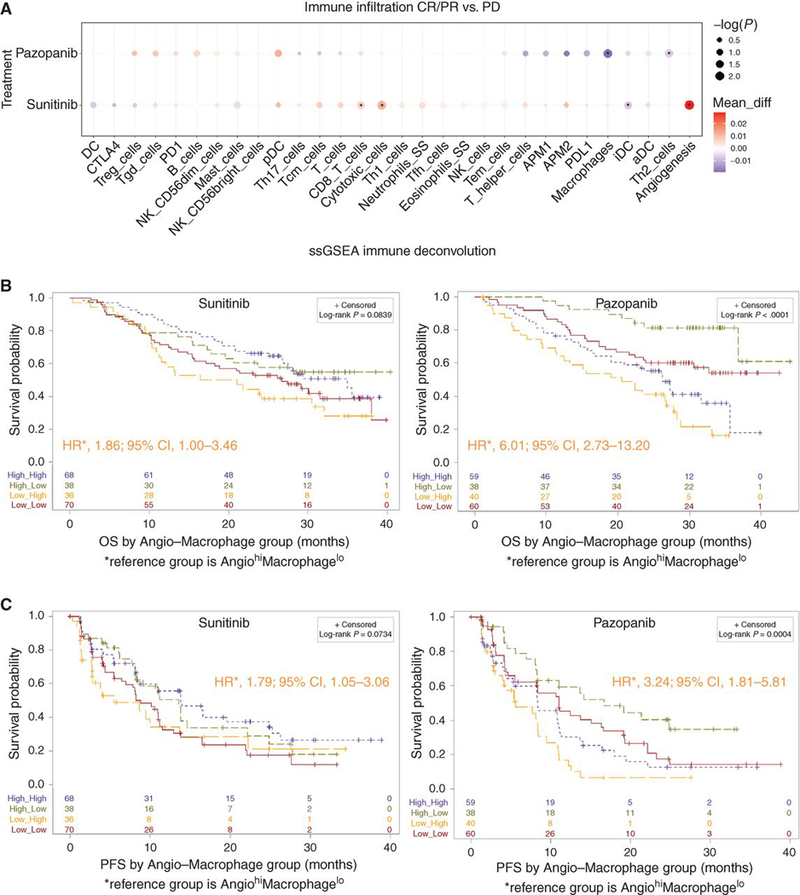
Metastasis remains the main reason for renal cell carcinoma (RCC)-associated mortality. Tyrosine kinase inhibitors (TKI) impart clinical benefit for most patients with RCC, but the determinants of response are poorly understood. We report an integrated genomic and transcriptomic analysis of patients with metastatic clear cell RCC (ccRCC) treated with TKI therapy and identify predictors of response. Patients in the COMPARZ phase III trial received first-line sunitinib or pazopanib with comparable efficacy. RNA-based analyses revealed four distinct molecular subgroups associated with response and survival. Characterization of these subgroups identified mutation profiles, angiogenesis, and macrophage infiltration programs to be powerful predictors of outcome with TKI therapy. Notably, predictors differed by the type of TKI received. Our study emphasizes the clinical significance of angiogenesis and immune tumor microenvironment and suggests that the critical effects its various aspects have on TKI efficacy vary by agent. This has broad implications for optimizing precision treatment of RCC. SIGNIFICANCE: The determinants of response to TKI therapy in metastatic ccRCC remain unknown. Our study demonstrates that key angiogenic and immune profiles of the tumor microenvironment may affect TKI response. These findings have the potential to inform treatment personalization in patients with RCC.This article is highlighted in the In This Issue feature, p. 453.
©2019 American Association for Cancer Research.
Figures
Comment in
-
The way towards tailored treatment for metastatic renal cancer patients in the omics era: are we getting a "transcriptomic compass"?Ann Transl Med. 2019 Sep;7(Suppl 6):S190. doi: 10.21037/atm.2019.07.37. Ann Transl Med. 2019. PMID: 31656769 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
