

Gut Microbiome Dysbiosis and Immunometabolism: New Frontiers for Treatment of Metabolic Diseases
- PMID: 30622429
- PMCID: PMC6304917
- DOI: 10.1155/2018/2037838
Gut Microbiome Dysbiosis and Immunometabolism: New Frontiers for Treatment of Metabolic Diseases
Abstract
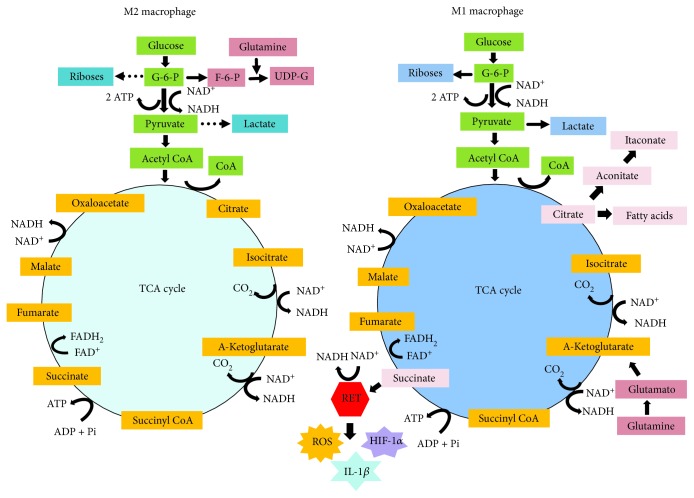
Maintenance of healthy human metabolism depends on a symbiotic consortium among bacteria, archaea, viruses, fungi, and host eukaryotic cells throughout the human gastrointestinal tract. Microbial communities provide the enzymatic machinery and the metabolic pathways that contribute to food digestion, xenobiotic metabolism, and production of a variety of bioactive molecules. These include vitamins, amino acids, short-chain fatty acids (SCFAs), and metabolites, which are essential for the interconnected pathways of glycolysis, the tricarboxylic acid/Krebs cycle, oxidative phosphorylation (OXPHOS), and amino acid and fatty acid metabolism. Recent studies have been elucidating how nutrients that fuel the metabolic processes impact on the ways immune cells, in particular, macrophages, respond to different stimuli under physiological and pathological conditions and become activated and acquire a specialized function. The two major inflammatory phenotypes of macrophages are controlled through differential consumption of glucose, glutamine, and oxygen. M1 phenotype is triggered by polarization signal from bacterial lipopolysaccharide (LPS) and Th1 proinflammatory cytokines such as interferon-γ, TNF-α, and IL-1β, or both, whereas M2 phenotype is triggered by Th2 cytokines such as interleukin-4 and interleukin-13 as well as anti-inflammatory cytokines, IL-10 and TGFβ, or glucocorticoids. Glucose utilization and production of chemical mediators including ATP, reactive oxygen species (ROS), nitric oxide (NO), and NADPH support effector activities of M1 macrophages. Dysbiosis is an imbalance of commensal and pathogenic bacteria and the production of microbial antigens and metabolites. It is now known that the gut microbiota-derived products induce low-grade inflammatory activation of tissue-resident macrophages and contribute to metabolic and degenerative diseases, including diabetes, obesity, metabolic syndrome, and cancer. Here, we update the potential interplay of host gut microbiome dysbiosis and metabolic diseases. We also summarize on advances on fecal therapy, probiotics, prebiotics, symbiotics, and nutrients and small molecule inhibitors of metabolic pathway enzymes as prophylactic and therapeutic agents for metabolic diseases.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
