

Principles of Immunotherapy: Implications for Treatment Strategies in Cancer and Infectious Diseases
- PMID: 30622524
- PMCID: PMC6308495
- DOI: 10.3389/fmicb.2018.03158
Principles of Immunotherapy: Implications for Treatment Strategies in Cancer and Infectious Diseases
Abstract
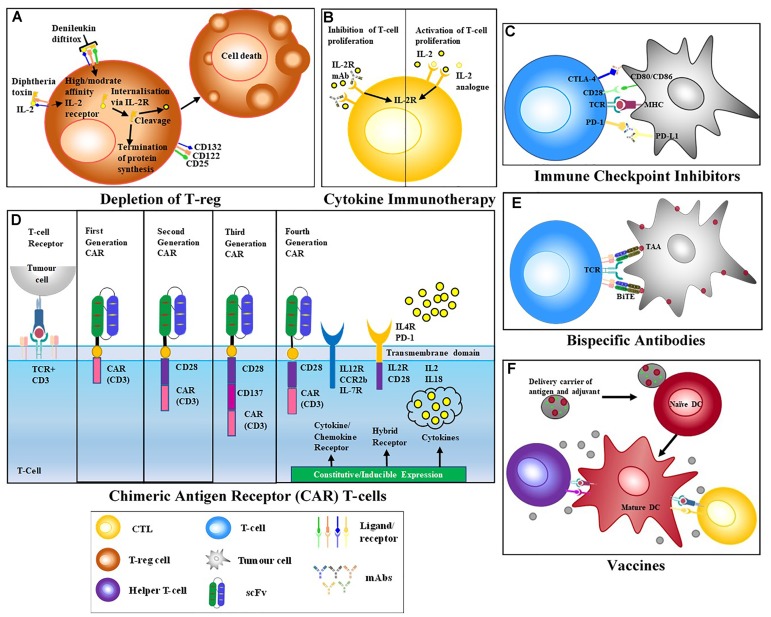
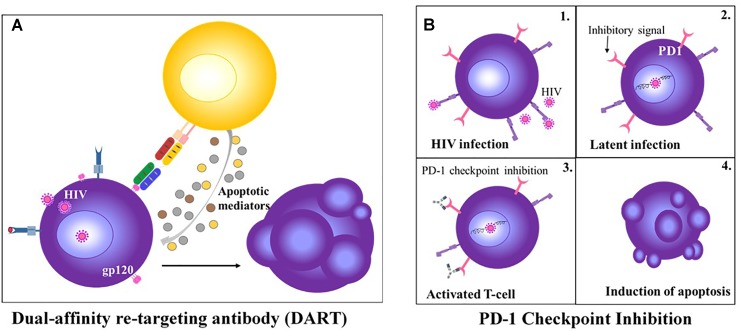
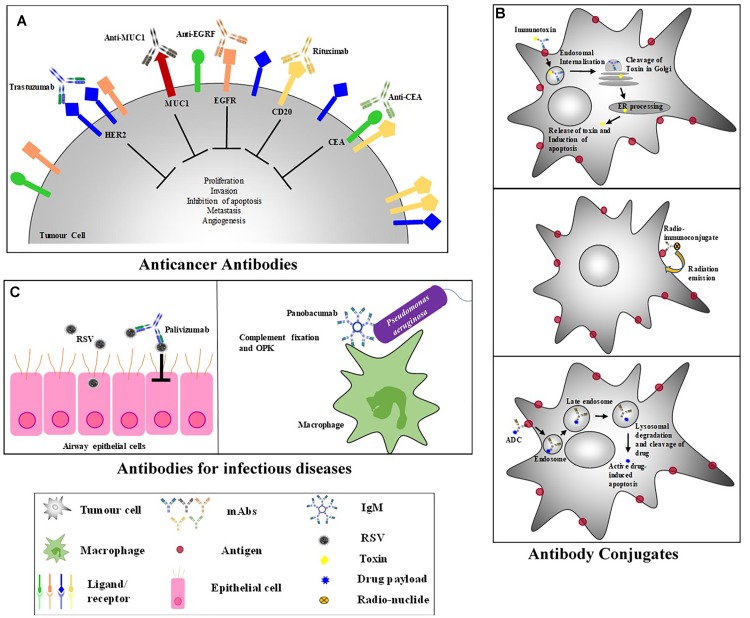
The advances in cancer biology and pathogenesis during the past two decades, have resulted in immunotherapeutic strategies that have revolutionized the treatment of malignancies, from relatively non-selective toxic agents to specific, mechanism-based therapies. Despite extensive global efforts, infectious diseases remain a leading cause of morbidity and mortality worldwide, necessitating novel, innovative therapeutics that address the current challenges of increasing antimicrobial resistance. Similar to cancer pathogenesis, infectious pathogens successfully fashion a hospitable environment within the host and modulate host metabolic functions to support their nutritional requirements, while suppressing host defenses by altering regulatory mechanisms. These parallels, and the advances made in targeted therapy in cancer, may inform the rational development of therapeutic interventions for infectious diseases. Although "immunotherapy" is habitually associated with the treatment of cancer, this review accentuates the evolving role of key targeted immune interventions that are approved, as well as those in development, for various cancers and infectious diseases. The general features of adoptive therapies, those that enhance T cell effector function, and ligand-based therapies, that neutralize or eliminate diseased cells, are discussed in the context of specific diseases that, to date, lack appropriate remedial treatment; cancer, HIV, TB, and drug-resistant bacterial and fungal infections. The remarkable diversity and versatility that distinguishes immunotherapy is emphasized, consequently establishing this approach within the armory of curative therapeutics, applicable across the disease spectrum.
Keywords: T cell therapy; antibody therapy; cancer; immunotherapy; infectious diseases.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous