

Distribution of the atypical pathogens of community-acquired pneumonia to disease severity
- PMID: 30622770
- PMCID: PMC6297405
- DOI: 10.21037/jtd.2018.10.50
Distribution of the atypical pathogens of community-acquired pneumonia to disease severity
Abstract
Background: To investigate the epidemiological characteristics of 11 atypical pathogens of community-acquired pneumonia (CAP) among Chinese, and to determine whether or not there is an association between these pathogens and the severity of illness.
Methods: We conducted a surveillance study for CAP in 30 hospitals of Beijing. Epidemiological data and clinical specimens were systematically collected from enrolled CAP patients. The detection for 11 atypical pathogens [9 respiratory viruses, Mycoplasma pneumoniae (MP) and Chlamydophila pneumoniae (CP)] was performed. Risk factors of severe CAP and death in Hospital were evaluated.
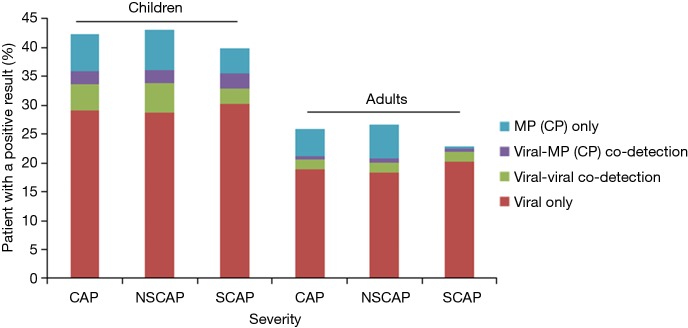
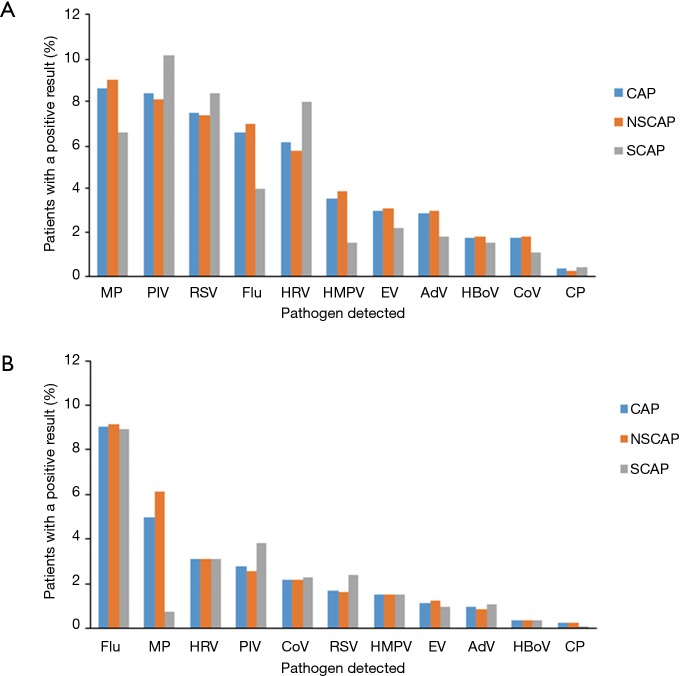
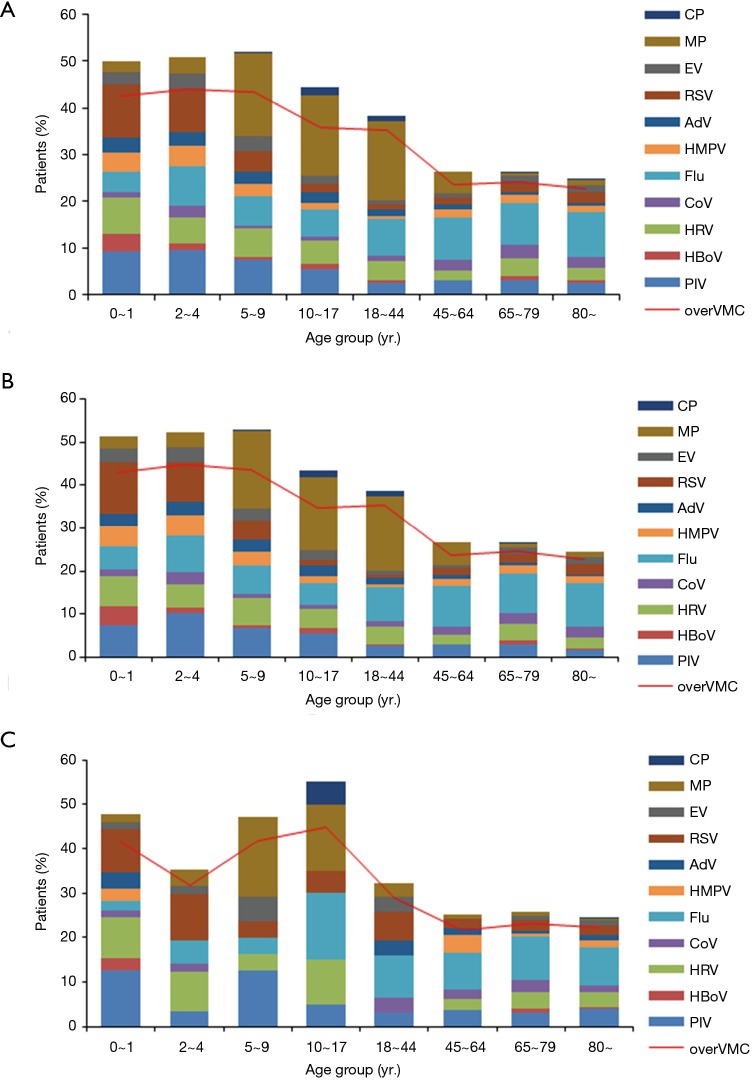
Results: A total of 6,008 CAP patients [including 1,071 severe CAP (SCAP)] were enrolled. The overall detection rate of the 11 atypical pathogens was 42.4% among 1,925 child CAP (39.9% among 274 child SCAP), and 25.8% among 4,083 adult CAP (22.8% among 797 adult SCAP). The most frequent atypical pathogen among child SCAP was parainfluenza virus (10.2%) followed by respiratory syncytial virus (RSV) (8.4%). However, the most frequent atypical pathogen among adult SCAP was influenza virus (8.9%) followed by parainfluenza virus (3.8%). Multivariate analyses showed that the important predictors for SCAP were an age ≤9 years, an age ≥65 years and co-existing diseases. These factors, except an age ≤9 years, were also predictors of death in Hospital. None of these 11 atypical pathogens was included as the risk factors of SCAP or death in Hospital.
Conclusions: Although these 11 atypical pathogens were the common causes of CAP (including SCAP) among Chinese, they were not observed to increase risks for SCAP or death in Hospital.
Keywords: Community-acquired pneumonia (CAP); atypical respiratory pathogen; respiratory pathogen; severe community acquired pneumonia; surveillance.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
-
- Marston BJ, Plouffe JF, File TM, Jr, et al. Incidence of community-acquired pneumonia requiring Hospitalization. Results of a population-based active surveillance Study in Ohio. The Community-Based Pneumonia Incidence Study Group. Arch Intern Med 1997;157:1709-18. 10.1001/archinte.1997.00440360129015 - DOI - PubMed
-
- Fielden NM. Community-acquired pneumonia. Perspect Respir Nurs 1998;9:1-2, 4, 6 passim. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous