

Recurrence of pectus excavatum following the Nuss procedure
- PMID: 30622792
- PMCID: PMC6297401
- DOI: 10.21037/jtd.2018.10.31
Recurrence of pectus excavatum following the Nuss procedure
Abstract
Background: The recurrence of pectus excavatum (PE), in other words, chest wall depression after the completion of repair, is one of the most important issues in PE. However, little about the recurrence of PE is known. The present study aimed (I) to evaluate the characteristics of chest wall depression during treatment and (II) to present the definition of recurrence of PE, investigate the risk factors for recurrence, and predict the recurrence at one year after bar removal (BR).
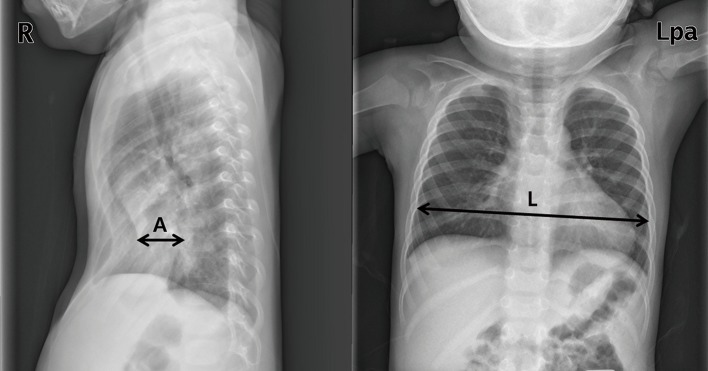
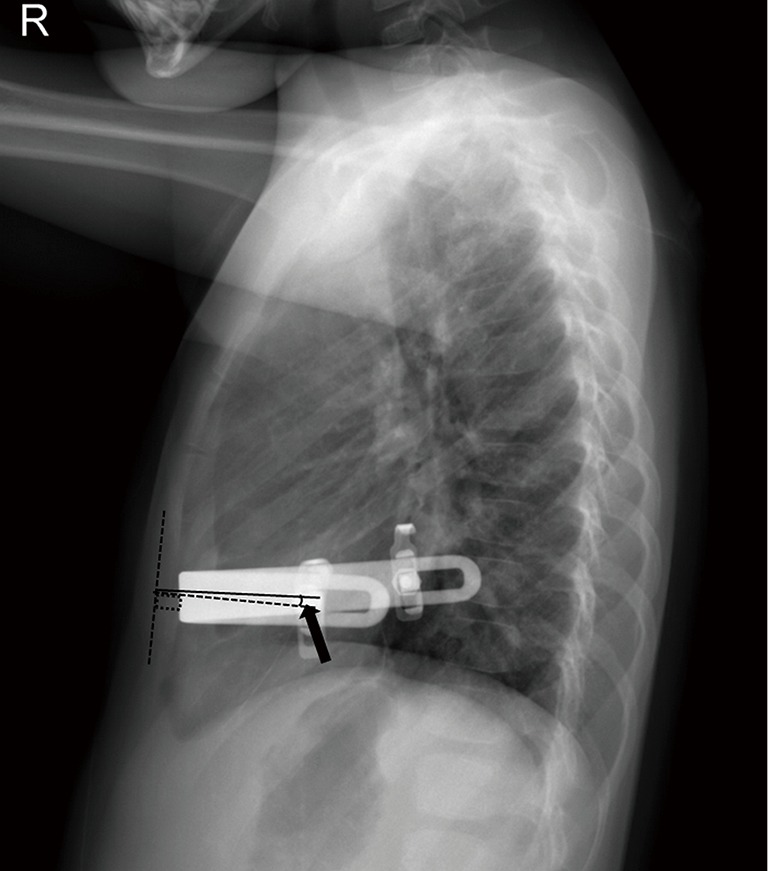
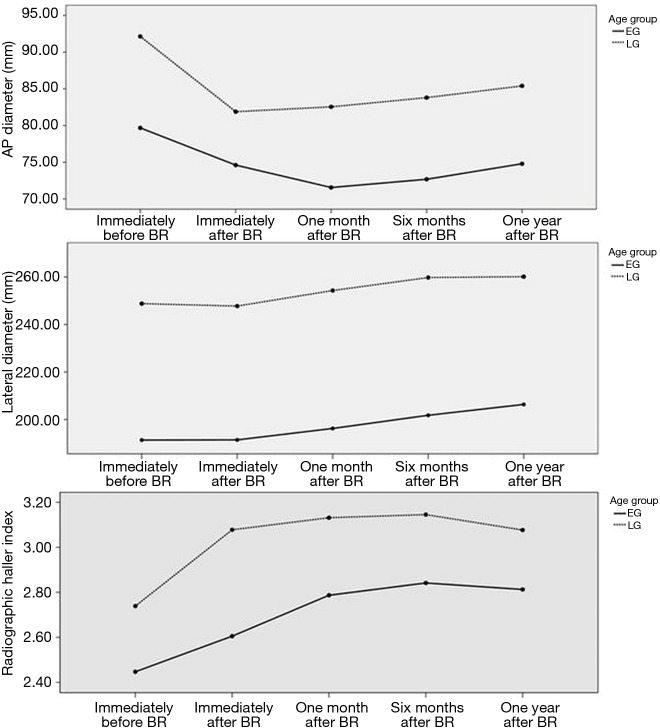
Methods: Consecutive 99 patients who had undergone BR for PE in a single hospital from March 2012 to June 2017 were included in the present study. Severity of PE is presented as a radiographical Haller index (RHI) in the present study. RHI is calculated by the ratio of the transverse diameter to the anteroposterior (AP) diameter at the point of the deepest chest wall depression. Patients with a ≥3.5 RHI value, which simultaneously increased to more than the value of RHI before BR, were considered as demonstrating recurrence in the present study. Follow-up data after BR were collected at subsequent time points (i.e., immediate before and after, one month, sixth months, and one year after BR). All postoperative chest wall changes were analyzed to find out the difference according to the age at the time of the Nuss procedure (NP) [<10 years old (early group; EG) vs. ≥10 years old (late group, LG)].
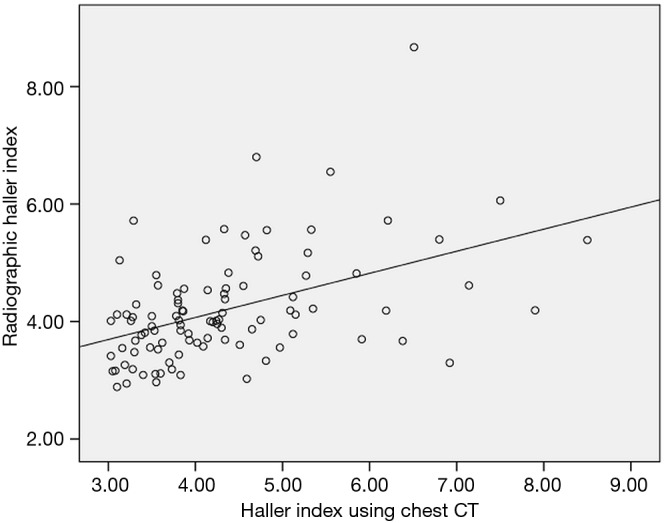
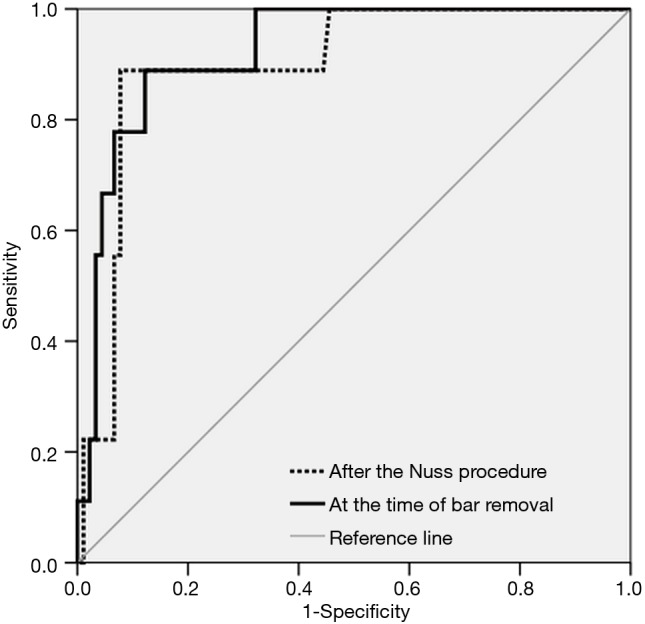
Results: The mean age of patients was 8.91 (±5.23) years at the age of the NP and the mean duration of bar placement was 28.4 (±5.04) months. Seventy-eight males and 21 females were included. The pectus type was 79 symmetric and 20 asymmetric cases. The mean observation period after BR was 16.47 (±3.74) months. There was a significant correlation between the Haller index using chest CT and simple radiography data (P<0.001). Irrespective of the age groups, there were a significant decrease in RHI values after the NP (both P<0.001). In addition, there were no differences in RHI values between the EG and the LG cohort before the NP and immediately after the NP (P=0.775, P=0.356, respectively). RHI values was significantly decreased in the EG (P=0.040) and increased without a significance in the LG (P=0.330) during bar placement. The chest wall depression progressed for the first six months after BR. However, the chest wall depression did not progress one year after BR. Recurrence occurred in nine cases at one year after BR (four cases in the EG and five cases in LG). The recurrence rate was higher in the LG than in the EG without a significance (P=0.479). Multivariate analysis of the recurrence revealed that only RHI after the NP was identified as an independent risk factor of the recurrence. ROC study also showed that RHI value after the NP had a significant predictable cutoff value for the recurrence [cutoff value of RHI: 2.91, sensitivity: 88.9%, specificity: 90.0%, P<0.001, area: 0.899, 95% confidence interval (CI): 0.806-0.993].
Conclusions: The present study shows the characteristics of chest wall depression and the risk factor of the recurrence of PE after BR. The effect of the NP is different according to the patient age at the time of the procedure. Early correction of PE can provide better corrective results because of the existence of a more pliable chest wall, which can be easily and sufficiently elevated by the NP. Sufficient elevation of the depressed chest wall should be ensured during the NP to prevent the recurrence of PE.
Keywords: Nuss procedure (NP); Pectus excavatum (PE); recurrence.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous