

Effects of Newer Antidiabetic Drugs on Endothelial Function and Arterial Stiffness: A Systematic Review and Meta-Analysis
- PMID: 30622967
- PMCID: PMC6304901
- DOI: 10.1155/2018/1232583
Effects of Newer Antidiabetic Drugs on Endothelial Function and Arterial Stiffness: A Systematic Review and Meta-Analysis
Abstract
Background: Newer antidiabetic drugs, i.e., dipeptidyl peptidase-4 (DPP-4) inhibitors, sodium-glucose cotransporter-2 (SGLT-2) inhibitors, and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) may exert distinct cardiovascular effects. We sought to explore their impact on vascular function.
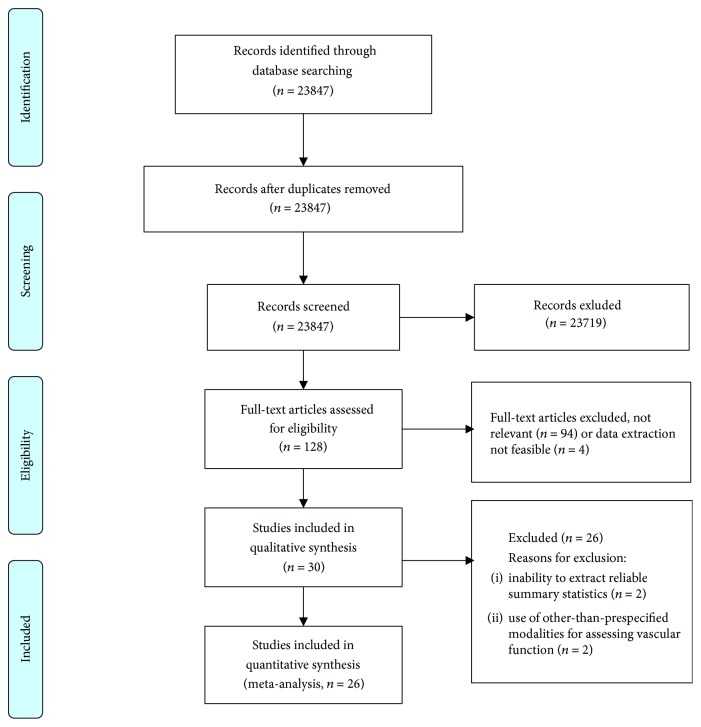
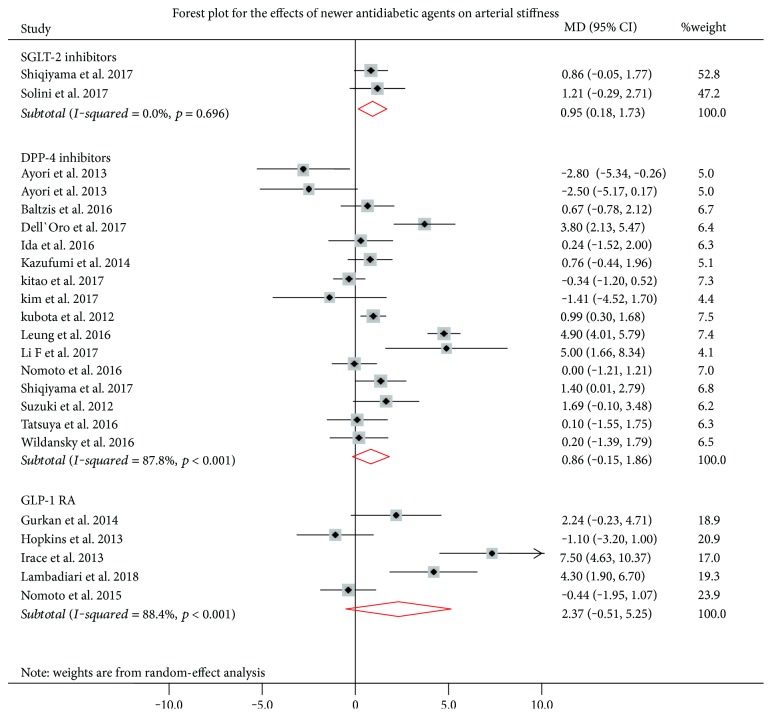
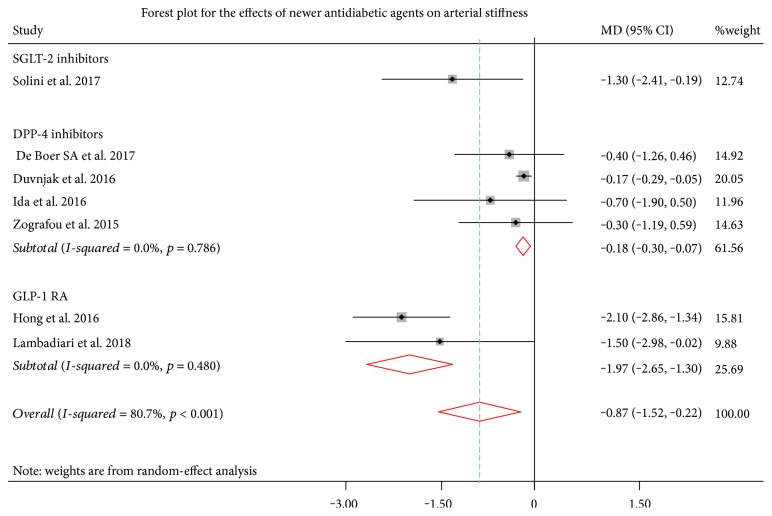
Methods: Published literature was systematically searched up to January 2018 for clinical studies assessing the effects of DPP-4 inhibitors, GLP-1 RAs, and SGLT-2 inhibitors on endothelial function and arterial stiffness, assessed by flow-mediated dilation (FMD) of the brachial artery and pulse wave velocity (PWV), respectively. For each eligible study, we used the mean difference (MD) with 95% confidence intervals (CIs) for FMD and PWV. The pooled MD for FMD and PWV were calculated by using a random-effect model. The presence of heterogeneity among studies was evaluated by the I 2 statistic.
Results: A total of 26 eligible studies (n = 668 patients) were included in the present meta-analysis. Among newer antidiabetic drugs, only SGLT-2 inhibitors significantly improved FMD (pooled MD 1.14%, 95% CI: 0.18 to 1.73, p = 0.016), but not DPP-4 inhibitors (pooled MD = 0.86%, 95% CI: -0.15 to 1.86, p = 0.095) or GLP-1 RA (pooled MD = 2.37%, 95% CI: -0.51 to 5.25, p = 0.107). Both GLP-1 RA (pooled MD = -1.97, 95% CI: -2.65 to -1.30, p < 0.001) and, to a lesser extent, DPP-4 inhibitors (pooled MD = -0.18, 95% CI: -0.30 to -0.07, p = 0.002) significantly decreased PWV.
Conclusions: Newer antidiabetic drugs differentially affect endothelial function and arterial stiffness, as assessed by FMD and PWV, respectively. These findings could explain the distinct effects of these drugs on cardiovascular risk of patients with type 2 diabetes.
Figures
References
-
- Low Wang C. C., Hess C. N., Hiatt W. R., Goldfine A. B. Clinical update: cardiovascular disease in diabetes mellitus. Atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus – mechanisms, management and clinical considerations. Circulation. 2016;133(24):2459–2502. doi: 10.1161/circulationaha.116.022194. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
