

Incidence of acute respiratory distress syndrome and associated mortality in a polytrauma population
- PMID: 30623025
- PMCID: PMC6307585
- DOI: 10.1136/tsaco-2018-000232
Incidence of acute respiratory distress syndrome and associated mortality in a polytrauma population
Abstract
Background: The incidence of acute respiratory distress syndrome (ARDS) has decreased in the last decade by improvement in trauma and critical care. However, it still remains a major cause of morbidity and mortality. This study investigated the current incidence and mortality of ARDS in polytrauma patients.
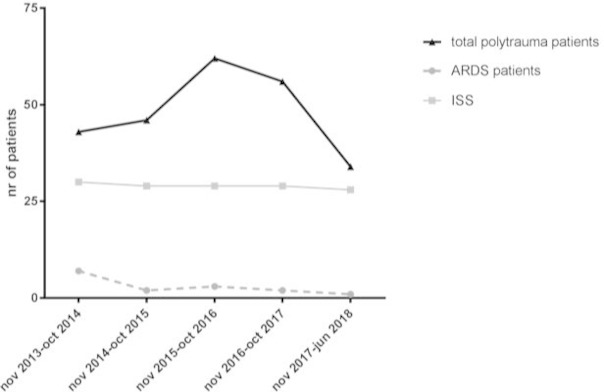
Methods: A 4.5-year prospective study included consecutive trauma patients admitted to a level 1 trauma center intensive care unit (ICU). Isolated head injuries, drowning, asphyxiation, burns, and deaths <48 hours were excluded. Demographics, Injury Severity Score (ISS), physiologic parameters, resuscitation parameters, Denver Multiple Organ Failure scores, and ARDS data according to Berlin criteria were prospectively collected. Data are presented as median (IQR), and p<0.05 was considered significant.
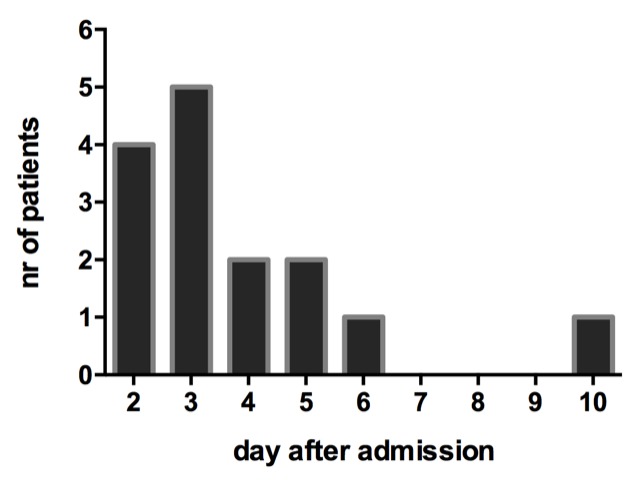
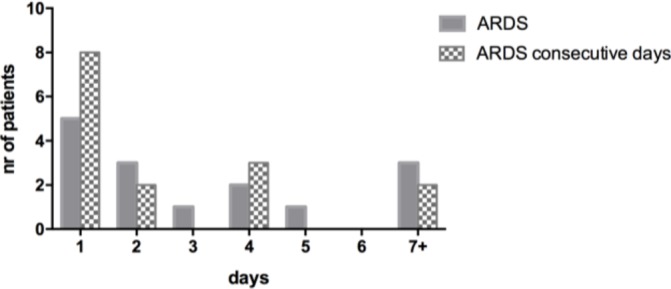
Results: 241 patients were included. The median age was 45 (27-59) years, 178 (74%) were male, the ISS was 29 (22-36), and 232 (96%) patients had blunt injuries. Thirty-one patients (13%) died. Fifteen patients (6%) developed ARDS. The median time to ARDS onset was 3 (2-5) days after injury. The median duration of ARDS was 2.5 (1-3.5) days. All patients with ARDS were male compared with 61% of non-ARDS patients (p=0.003). Patients who developed ARDS had higher ISS (30 vs. 25, p=0.01), lower Partial Pressure of Oxygen in arterial blood (PaO2) both in the emergency department and ICU, and higher Partial Pressure of Carbon Dioxide in arterial blood (PaCo2) in the ICU. Patients with ARDS needed more crystalloids <24 hours (8.7 vs. 6.8 L, p=0.03), received more fresh frozen plasma <24 hours (3 vs. 0 U, p=0.04), and more platelet <8 hours and <24 hours. Further, they stayed longer on the ventilator (11 vs. 2 days, p<0.001), longer in the ICU (12 vs. 3 days, p<0.001), and in the hospital (33 vs. 15 days, p=0.004). Patients with ARDS developed more often multiple organ dysfunction syndrome (40% vs. 3%, p<0.001) and died more often (20% vs. 3%, p=0.01). Only one patient with ARDS (7%) died of ARDS.
Discussion: In this polytrauma population mortality was predominantly caused by brain injury. The incidence of ARDS was low; its presentation was only early onset, during a short time period, and accompanied by low mortality.
Level of evidence: Level III.
Keywords: ARDS; mortality; polytrauma.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Attenuation of MODS-related and ARDS-related mortality makes infectious complications a remaining challenge in the severely injured.Trauma Surg Acute Care Open. 2020 Feb 4;5(1):e000398. doi: 10.1136/tsaco-2019-000398. eCollection 2020. Trauma Surg Acute Care Open. 2020. PMID: 32154377 Free PMC article.
-
Reduction in Mortality Rates of Postinjury Multiple Organ Dysfunction Syndrome: A Shifting Paradigm? A Prospective Population-Based Cohort Study.Shock. 2018 Jan;49(1):33-38. doi: 10.1097/SHK.0000000000000938. Shock. 2018. PMID: 28682941
-
Is chest imaging relevant in diagnosing acute respiratory distress syndrome in polytrauma patients? A population-based cohort study.Eur J Trauma Emerg Surg. 2020 Dec;46(6):1393-1402. doi: 10.1007/s00068-019-01204-3. Epub 2019 Aug 10. Eur J Trauma Emerg Surg. 2020. PMID: 31401658 Free PMC article.
-
Dilemma of crystalloid resuscitation in non-exsanguinating polytrauma: what is too much?Trauma Surg Acute Care Open. 2020 Oct 28;5(1):e000593. doi: 10.1136/tsaco-2020-000593. eCollection 2020. Trauma Surg Acute Care Open. 2020. PMID: 33178897 Free PMC article.
-
Mortality of Adult Respiratory Distress Syndrome in Trauma Patients: A Systematic Review over a Period of Four Decades.World J Surg. 2020 Jul;44(7):2243-2254. doi: 10.1007/s00268-020-05483-5. World J Surg. 2020. PMID: 32179975
Cited by
-
Inflammation, Thrombosis, and Destruction: The Three-Headed Cerberus of Trauma- and SARS-CoV-2-Induced ARDS.Front Immunol. 2020 Sep 25;11:584514. doi: 10.3389/fimmu.2020.584514. eCollection 2020. Front Immunol. 2020. PMID: 33101314 Free PMC article. Review.
-
Effect of Injury Patterns on the Development of Complications and Trauma-Induced Mortality in Patients Suffering Multiple Trauma.J Clin Med. 2023 Aug 3;12(15):5111. doi: 10.3390/jcm12155111. J Clin Med. 2023. PMID: 37568511 Free PMC article.
-
TBI related death has become the new epidemic in polytrauma: a 10-year prospective cohort analysis in severely injured patients.Eur J Trauma Emerg Surg. 2024 Dec;50(6):3083-3094. doi: 10.1007/s00068-024-02653-1. Epub 2024 Sep 17. Eur J Trauma Emerg Surg. 2024. PMID: 39287678 Free PMC article.
-
The evolution of trauma care in the Netherlands over 20 years.Eur J Trauma Emerg Surg. 2020 Apr;46(2):329-335. doi: 10.1007/s00068-019-01273-4. Epub 2019 Nov 23. Eur J Trauma Emerg Surg. 2020. PMID: 31760466 Free PMC article. Review.
-
Attenuation of MODS-related and ARDS-related mortality makes infectious complications a remaining challenge in the severely injured.Trauma Surg Acute Care Open. 2020 Feb 4;5(1):e000398. doi: 10.1136/tsaco-2019-000398. eCollection 2020. Trauma Surg Acute Care Open. 2020. PMID: 32154377 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials