

Age-Specific Cutoffs of the Sysmex UF-1000i Automated Urine Analyzer for Rapid Screening of Urinary Tract Infections in Outpatients
- PMID: 30623625
- PMCID: PMC6340846
- DOI: 10.3343/alm.2019.39.3.322
Age-Specific Cutoffs of the Sysmex UF-1000i Automated Urine Analyzer for Rapid Screening of Urinary Tract Infections in Outpatients
Abstract
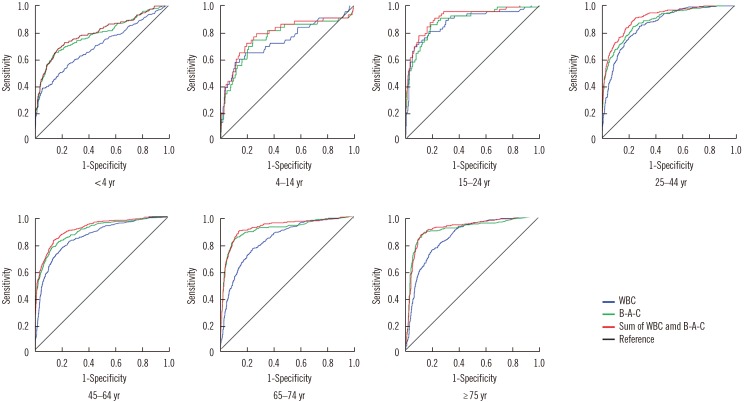
We investigated the usefulness of age-specific cutoffs for screening of urinary tract infections (UTIs) in Korean outpatients, using the automated urine analyzer UF-1000i (Sysmex, Kobe, Japan). We retrospectively reviewed outpatient medical records. Urine samples of 7,443 outpatients from January 2010 to December 2017 were analyzed using urine culture and UF-1000i. ROC curves were calculated for each UF-1000i parameter based on the culture results. There were 1,398 culture positive samples, 5,774 culture negative samples, and 271 contaminated samples. UF-1000i had an area under the curve of ≥0.9 in outpatients >15 years. The appropriate cutoffs, which are the sum of bacterial (B-A-C) and white blood cell (WBC) counts, were 297.10/μL (15-24 years), 395.65/μL (25-44 years), 135.65/μL (45-64 years), 67.95/μL (65-74 years), and 96.5/μL (≥75 years). B-A-C and WBC counts differed among the three most frequently identified bacteria (Escherichia coli, Klebsiella pneumoniae, and Enterococcus faecalis). The UF-1000i system is useful for applying age-specific cutoffs to screen for UTIs, thereby preventing antibiotic abuse and reducing antibiotic resistance. Future studies can explore how its B-A-C and WBC counts can facilitate selection of empirical antibiotics by distinguishing between gram-positive and gram-negative bacteria.
Keywords: Age-specific cutoff; Outpatients; UF-1000i; Urinary tract infection.
© The Korean Society for Laboratory Medicine.
Conflict of interest statement
No potential conflicts of interest relevant to this article are reported.
Figures

References
-
- Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 2001;183(S1):S1–S4. - PubMed
-
- Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for 2007. Vital Health Stat 13. 2011 Apr;:1–38. - PubMed
-
- Huh JS. The prevalence of urinary tract infections in institutionalized vs. noninstitutionalized elderly persons. Urogenit Tract Infect. 2016;11:56–61.
-
- Lee KY. New insights for febrile urinary tract infection (acute pyelonephritis) in children. Child Kidney Dis. 2016;20:37–44.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
