

Continuous Electroencephalography After Moderate to Severe Traumatic Brain Injury
- PMID: 30624278
- PMCID: PMC6639805
- DOI: 10.1097/CCM.0000000000003639
Continuous Electroencephalography After Moderate to Severe Traumatic Brain Injury
Abstract
Objectives: After traumatic brain injury, continuous electroencephalography is widely used to detect electrographic seizures. With the development of standardized continuous electroencephalography terminology, we aimed to describe the prevalence and burden of ictal-interictal patterns, including electrographic seizures after moderate-to-severe traumatic brain injury and to correlate continuous electroencephalography features with functional outcome.
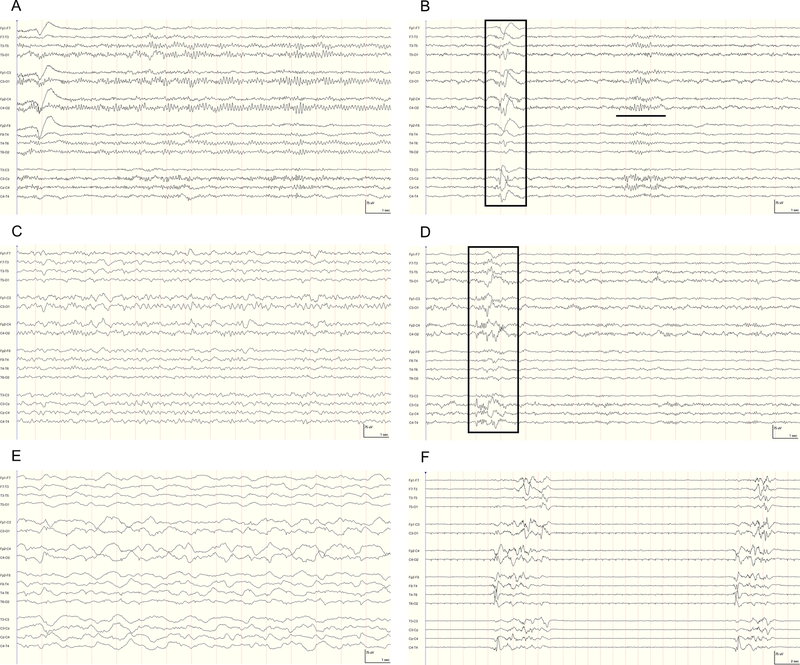
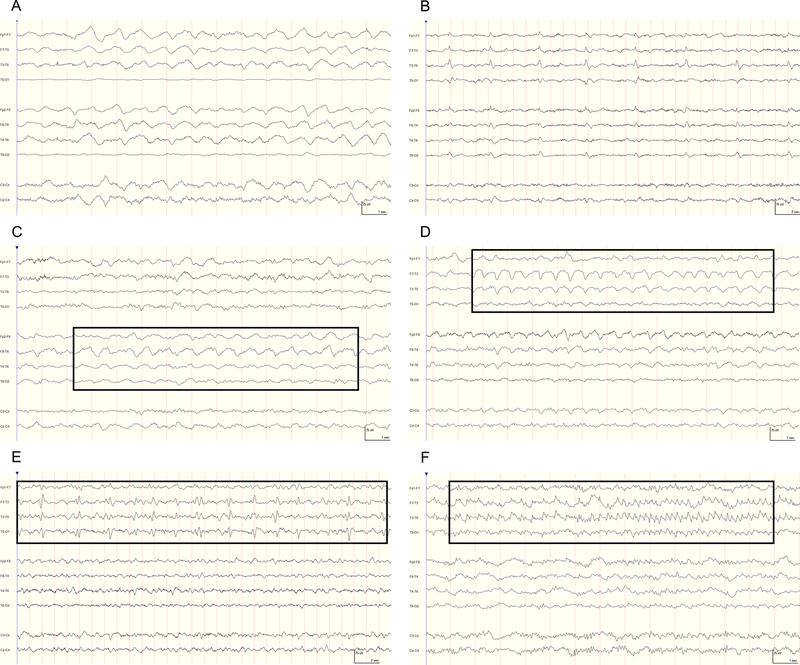
Design: Post hoc analysis of the prospective, randomized controlled phase 2 multicenter INTREPID study (ClinicalTrials.gov: NCT00805818). Continuous electroencephalography was initiated upon admission to the ICU. The primary outcome was the 3-month Glasgow Outcome Scale-Extended. Consensus electroencephalography reviews were performed by raters certified in standardized continuous electroencephalography terminology blinded to clinical data. Rhythmic, periodic, or ictal patterns were referred to as "ictal-interictal continuum"; severe ictal-interictal continuum was defined as greater than or equal to 1.5 Hz lateralized rhythmic delta activity or generalized periodic discharges and any lateralized periodic discharges or electrographic seizures.
Setting: Twenty U.S. level I trauma centers.
Patients: Patients with nonpenetrating traumatic brain injury and postresuscitation Glasgow Coma Scale score of 4-12 were included.
Interventions: None.
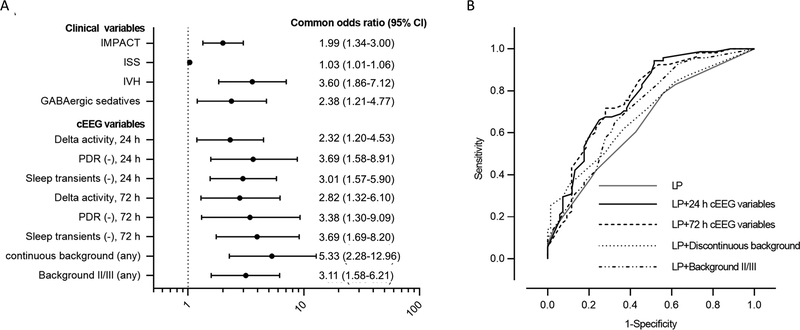
Measurements and main results: Among 152 patients with continuous electroencephalography (age 34 ± 14 yr; 88% male), 22 (14%) had severe ictal-interictal continuum including electrographic seizures in four (2.6%). Severe ictal-interictal continuum burden correlated with initial prognostic scores, including the International Mission for Prognosis and Analysis of Clinical Trials in Traumatic Brain Injury (r = 0.51; p = 0.01) and Injury Severity Score (r = 0.49; p = 0.01), but not with functional outcome. After controlling clinical covariates, unfavorable outcome was independently associated with absence of posterior dominant rhythm (common odds ratio, 3.38; 95% CI, 1.30-9.09), absence of N2 sleep transients (3.69; 1.69-8.20), predominant delta activity (2.82; 1.32-6.10), and discontinuous background (5.33; 2.28-12.96) within the first 72 hours of monitoring.
Conclusions: Severe ictal-interictal continuum patterns, including electrographic seizures, were associated with clinical markers of injury severity but not functional outcome in this prospective cohort of patients with moderate-to-severe traumatic brain injury. Importantly, continuous electroencephalography background features were independently associated with functional outcome and improved the area under the curve of existing, validated predictive models.
Figures
References
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. The Journal of head trauma rehabilitation. 2006. Sep-Oct;21(5):375–8. - PubMed
-
- Hukkelhoven CW, Steyerberg EW, Habbema JD, et al. Predicting outcome after traumatic brain injury: development and validation of a prognostic score based on admission characteristics. Journal of neurotrauma. 2005. October;22(10):1025–39. - PubMed
-
- Husson EC, Ribbers GM, Willemse-van Son AH, Verhagen AP, Stam HJ. Prognosis of six-month functioning after moderate to severe traumatic brain injury: a systematic review of prospective cohort studies. Journal of rehabilitation medicine. 2010. May;42(5):425–36. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
