

Comorbidity, Frailty, and Waitlist Mortality among Kidney Transplant Candidates of All Ages
- PMID: 30625489
- PMCID: PMC6374203
- DOI: 10.1159/000496061
Comorbidity, Frailty, and Waitlist Mortality among Kidney Transplant Candidates of All Ages
Abstract
Background: Kidney transplantation (KT) candidates often present with multiple comorbidities. These patients also have a substantial burden of frailty, which is also associated with increased mortality. However, it is unknown if frailty is merely a surrogate for comorbidity, itself an independent domain of risk, or if frailty and comorbidity have differential effects. Better understanding the interplay between these 2 constructs will improve clinical decision making in KT candidates.
Objective: To test whether comorbidity is equally associated with waitlist mortality among frail and nonfrail KT candidates and to test whether measuring both comorbidity burden and frailty improves mortality risk prediction.
Methods: We studied 2,086 candidates on the KT waitlist (November 2009 - October 2017) in a multicenter cohort study, in whom frailty and comorbidity were measured at evaluation. We quantified the association between Charlson comorbidity index (CCI) adapted for end-stage renal disease and waitlist mortality using an adjusted Cox proportional hazards model and tested whether this association differed between frail and nonfrail candidates.
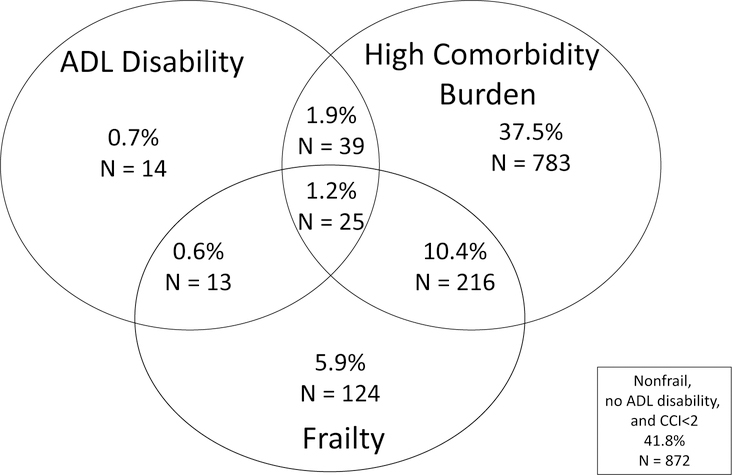
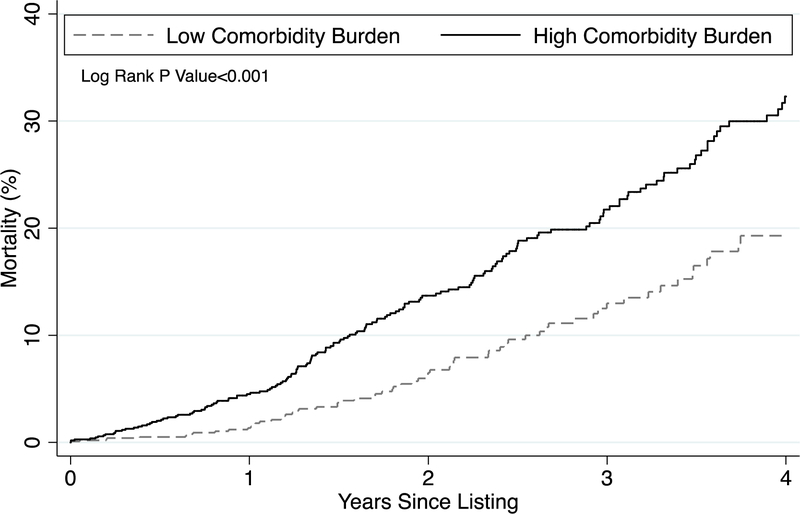
Results: At evaluation, 18.1% of KT candidates were frail and 51% had a high comorbidity burden (CCI score ≥2). Candidates with a high comorbidity burden were at 1.38-fold (95% CI 1.01-1.89) increased risk of waitlist mortality. However, this association differed by frailty status (p for interaction = 0.01): among nonfrail candidates, a high comorbidity burden was associated with a 1.66-fold (95% CI 1.17-2.35) increased mortality risk; among frail candidates, here was no statistically significant association (HR 0.75, 95% CI 0.44-1.29). Adding this interaction between comorbidity and frailty to a mortality risk estimation model significantly improved prediction, increasing the c-statistic from 0.640 to 0.656 (p < 0.001).
Conclusions: Nonfrail candidates with a high comorbidity burden at KT evaluation have an increased risk of waitlist mortality. Importantly, comorbidity is less of a concern in already high-risk patients who are frail.
Keywords: Comorbidity; Frailty; Kidney transplantation.
© 2019 S. Karger AG, Basel.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
None. The results presented in this paper have not been published previously in whole or part, except in abstract format.
Figures
References
-
- Keane WF, Collins AJ. Influence of co-morbidity on mortality and morbidity in patients treated with hemodialysis. Am J Kidney Dis 1994;24(6):1010–8. - PubMed
-
- Khan IH, Catto GR, Edward N, et al. Influence of coexisting disease on survival on renal-replacement therapy. Lancet 1993;341(8842):415–8. - PubMed
-
- Miskulin DC, Athienites NV, Yan G, et al. Comorbidity assessment using the Index of Coexistent Diseases in a multicenter clinical trial. Kidney Int 2001;60(4):1498–510. - PubMed
-
- Hemmelgarn BR, Manns BJ, Quan H, et al. Adapting the Charlson Comorbidity Index for use in patients with ESRD. Am J Kidney Dis 2003;42(1):125–32. - PubMed
-
- Jassal SV, Schaubel DE, Fenton SS. Baseline comorbidity in kidney transplant recipients: a comparison of comorbidity indices. Am J Kidney Dis 2005;46(1):136–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
