

The improvement in neurocognitive functioning in anorexia nervosa adolescents throughout the integrative model of psychotherapy including cognitive remediation therapy
- PMID: 30626367
- PMCID: PMC6327421
- DOI: 10.1186/s12888-018-1984-4
The improvement in neurocognitive functioning in anorexia nervosa adolescents throughout the integrative model of psychotherapy including cognitive remediation therapy
Abstract
Background: Patients with anorexia nervosa (AN) experience difficulties in neurocognitive functioning in the acute phase of illness which might be related to clinical presentation, but also in the apparently remitted state after weight recovery. Among the most commonly reported persistent deficits is cognitive inflexibility, which can be interpreted as a vulnerability trait or a "neuropsychological scar" reflecting the detrimental effect of prolonged semi-starvation in patients with a long duration of illness. Studies of adolescent samples with a relatively short clinical course may enable avoiding the effect of prolonged illness and help to determine whether neuropsychological deficits are trait or state dependent. The aim of this study is to assess cognitive functioning in adolescents with AN before and after the inpatient treatment programme, including cognitive remediation therapy (CRT).
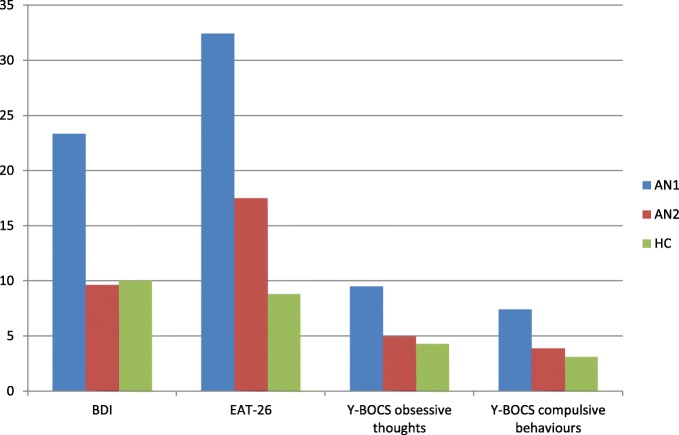
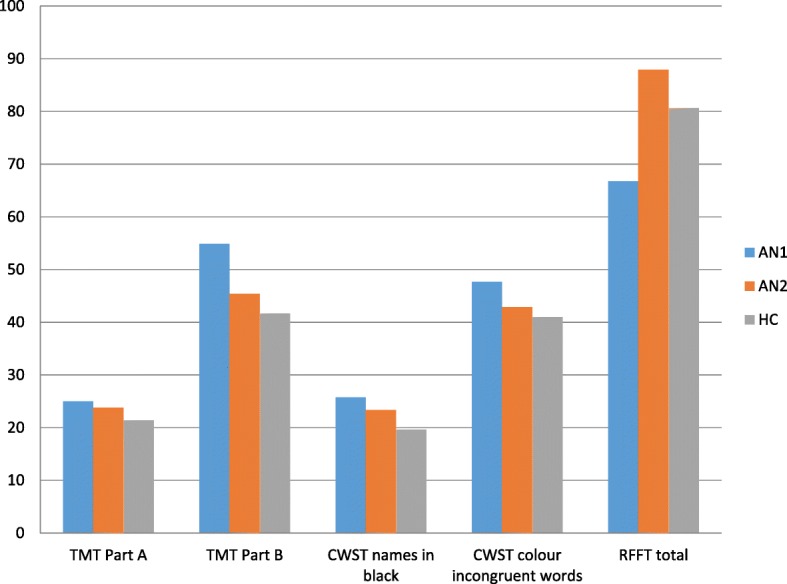
Methods: Forty-seven adolescent female inpatients with AN diagnosed according to DSM-5 and fifty healthy female adolescents matched for the education level and age were recruited. The patients underwent a multimodal treatment including a ten-week CRT. The standardized and cross-validated neuropsychological (Trail Making Test - TMT A and B, Color-Word Stroop Task - CWST, Ruff Figural Fluency Test - RFFT) and clinical measurements (Beck Depression Inventory - BDI, Eating Attitude Test - EAT-26, Yale-Brown Obsessive Compulsive Scale - Y-BOCS) were used to assess both clinical (in the acute phase and after partial weight recovery) and control subjects.
Results: Initially, AN patients performed significantly worse compared to the controls, but afterwards, inpatient treatment improvement was noted on all examined measures. In a few subtests (TMT, CWST) performance of AN patients after the programme was still significantly poorer than in HC.
Conclusions: Cognitive inflexibility in adolescent AN patients, as measured with TMT, CWST, and RFFT tends to improve after therapy. Nevertheless, a few neuropsychological subtests which did not show complete normalization may warrant attention in subsequent studies. Further research including control intervention is needed to conclude whether CRT intervention affects the outcome.
Keywords: Anorexia nervosa; Cognitive remediation therapy; Neurocognition; Psychotherapy.
Conflict of interest statement
Ethics approval and consent to participate
Study was conducted at the Department of Child and Adolescent Psychiatry in The Institute of Psychiatry and Neurology in Warsaw, Poland; Principal Investigator—Prof. K. Kucharska.
Patients were assessed after giving informed written consent. Informed written consent of participation in the study were obtained from all participants (or their parent or legal guardian in the case of children under 16). Approval for the study was obtained from the ethics committee of the Institute of Psychiatry and Neurology in Warsaw, Poland on 26th February 2015 (reference number 7/2015 KB IPiN).
Competing interests
The authors declare that they have no competing interests.
This research is supported by National Centre of Science (NCN) (Grant No. 2014/15/B/HS6/01847).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Hamsher Kde S, Halmi KA, Benton AL. Prediction of outcome in anorexia nervosa from neuropsychological status. Psychiatry Res. 1981;4(1):79–88. - PubMed
-
- Boersma GJ, Treesukosol Y, Cordner ZA, Kastelein A, Choi P, Moran TH, Tamashiro KL. Exposure to activity-based anorexia impairs contextual learning in weight-restored rats without affecting spatial learning, taste, anxiety, or dietary-fat preference. Int J Eat Disord. 2016;49(2):167–179. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
