

Pre-hospital management of acute stroke patients eligible for thrombolysis - an evaluation of ambulance on-scene time
- PMID: 30626404
- PMCID: PMC6327613
- DOI: 10.1186/s13049-018-0580-4
Pre-hospital management of acute stroke patients eligible for thrombolysis - an evaluation of ambulance on-scene time
Abstract
Background: Stroke is a leading cause of death and disability with effective treatment, including thrombolysis or thrombectomy, being time-critical for favourable outcomes. While door-to-needle time in hospital has been optimized for many years, little is known about the ambulance on-scene time (OST). OST has been reported to account for 44% of total alarm-to-door time, thereby being a major time component. We aimed to analyse ambulance OST in stroke patients eligible for thrombolysis and identify potential areas of time optimization.
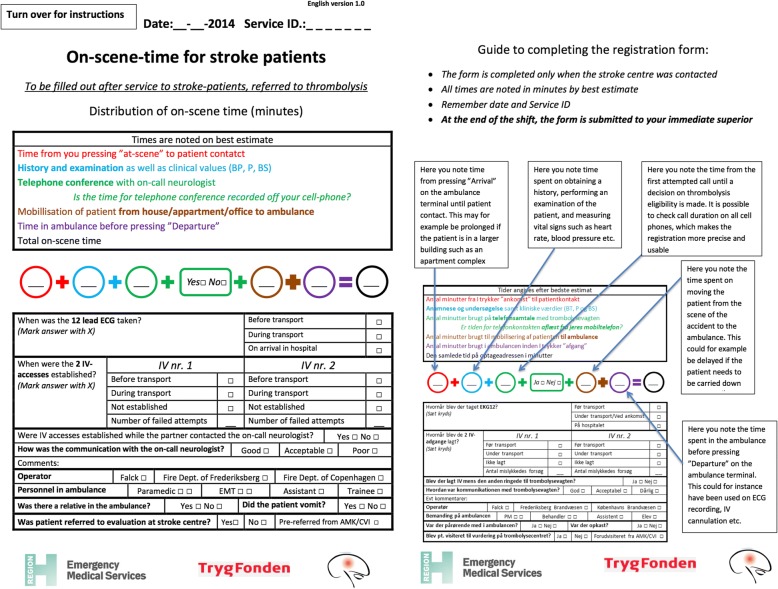
Methods: A study-specific registration form was developed to record detailed information about OST consumption in cases where the Emergency Medical Services (EMS) suspected a stroke from July 2014-May 2015. Registration forms were completed by ambulance personnel and included details on estimated time spent: 1) localising patient, 2) clinical examination, 3) consulting with the on-call neurologist, 4) mobilising patient to the ambulance, 5) treatment in ambulance before departure. Additionally, estimated total OST was noted. For patients found eligible for further evaluation at a stroke centre, time points were analysed using multivariate Poisson regressions.
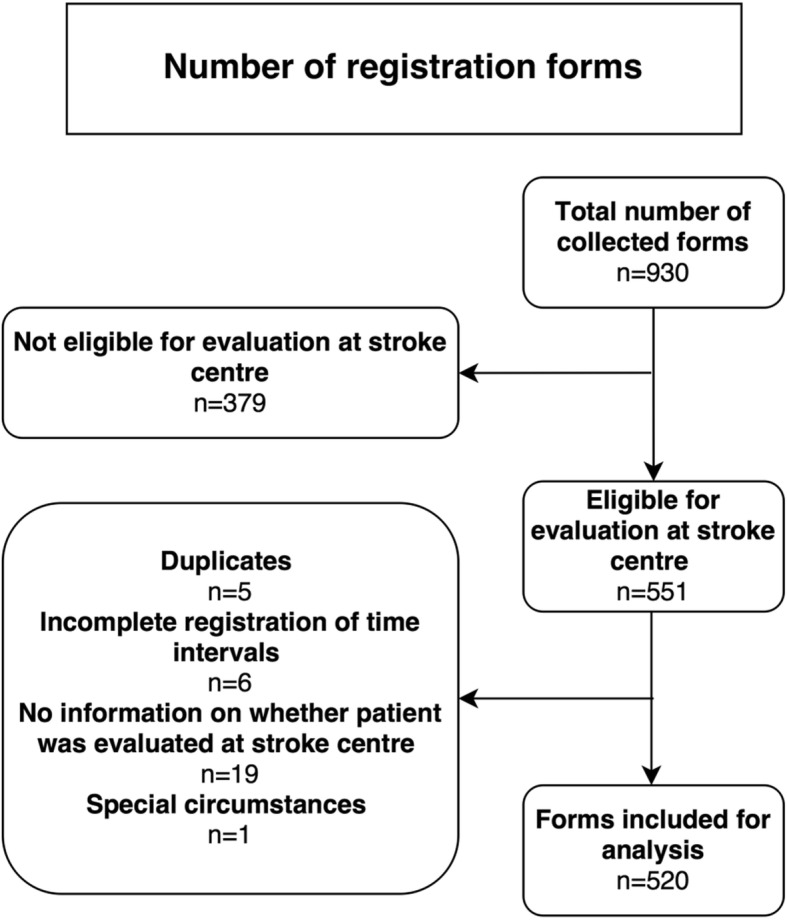
Results: A total of 520 cases were included. The median OST was 21 min (Interquartile Range (IQR) 16-27). Time consumption was significantly lower (17 vs 21 min, p = 0.0015) when electrocardiography (ECG) was obtained in-hospital instead of on-scene, when intravenous (IV) access was established during transportation instead of before transportation (17 vs 21 min, p < 0.0001), and when the quality of communication with the stroke centres was rated as "good" as opposed to "acceptable/poor" (21 vs 23 min, p = 0.014). Neither the presence of relatives nor ambulance trainees had a significant effect on OST.
Conclusions: In-hospital ECG recording and IV cannulation during transport were found to reduce OST, while "acceptable/poor" communication was found to prolong OST relative to "good" communication. These components of pre-hospital stroke management represent potential opportunities for lowering OST with relatively simple changes, which could ultimately lead to earlier treatment and better patient outcome.
Trial registration: Unique identifier: NCT02191514 .
Keywords: Cerebrovascular disease; Emergency medical services; Ischemic stroke; Pre-hospital delay; Pre-hospital stroke management; Stroke; Stroke on-scene time; Thrombolysis.
Conflict of interest statement
Ethics approval and consent to participate
Approval from the Danish Data Protection Agency (2007-58-0015) was obtained. Approval from the regional ethics committee was not required (H-4-2014-FSP).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO. The top 10 causes of death. Available from: http://www.who.int/gho/mortality_burden_disease/causes_death/top_10/en/. Accessed 29th October 2018.
-
- Centers for Disease Control and Prevention. Stroke Fact Sheet. Available from: https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_stroke.htm. Accessed 29th October 2018.
-
- Dansk Selskab for Apopleksi. Referenceprogram for behandling af patienter med apopleksi 2012. Available from: http://www.dsfa.dk/wp-content/uploads/REFERENCEPROGRAMFINAL20131.pdf. Accessed: 27th October 2018.
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
