

Natural Inhibitor of Human Cytomegalovirus in Human Seminal Plasma
- PMID: 30626669
- PMCID: PMC6401442
- DOI: 10.1128/JVI.01855-18
Natural Inhibitor of Human Cytomegalovirus in Human Seminal Plasma
Abstract
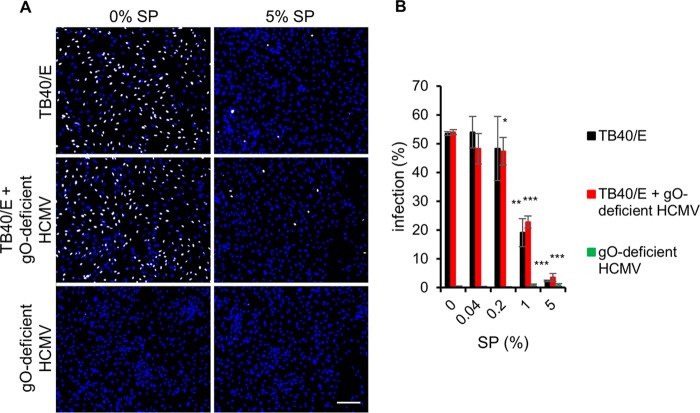
Human cytomegalovirus (HCMV) is the most frequent viral cause of congenital infections that can lead to severe birth defects. Although HCMV is frequently detected in semen and thus is potentially sexually transmitted, the role of semen in HCMV transmission is largely unclear. Here we describe that human seminal plasma (SP; the cell-free supernatant of semen) inhibits HCMV infection. The inhibition of HCMV infection was dose dependent and effective for different cell types, virus strains, and semen donors. This inhibitory effect was specific for HCMV, as herpes simplex virus 2 (HSV-2) and human immunodeficiency virus type 1 (HIV-1) infections were enhanced by SP. Mechanistically, SP inhibited infection by interfering with the attachment of virions to cells most likely via an interaction with the trimeric glycoprotein complex gH/gL/gO. Together, our findings suggest that semen contains a factor that potentially limits sexual transmission of HCMV.IMPORTANCE The role of semen in sexual transmission of human cytomegalovirus (HCMV) is currently unclear. This is surprising, as HCMV is frequently detected in this body fluid and infection is of high danger for neonates and pregnant women. In this study, we found that seminal plasma (SP) dose dependently inhibited HCMV infection. The infection inhibition was specific for HCMV, as other viruses, such as human immunodeficiency virus type 1 (HIV-1) and herpes simplex virus 2 (HSV-2), were not inhibited by SP. SP must contain a soluble, heat-resistant factor that limits attachment of HCMV particles to cells, probably by interaction with the trimeric glycoprotein complex gH/gL/gO. This novel virus-host interaction could possibly limit transmission of HCMV via semen during sexual intercourse.
Keywords: HCMV; SEVI; attachment; gH/gL/gO; glycoprotein O; human cytomegalovirus; semen; seminal amyloids; sexual transmission.
Copyright © 2019 American Society for Microbiology.
Figures









Similar articles
-
Monoclonal Antibodies to Different Components of the Human Cytomegalovirus (HCMV) Pentamer gH/gL/pUL128L and Trimer gH/gL/gO as well as Antibodies Elicited during Primary HCMV Infection Prevent Epithelial Cell Syncytium Formation.J Virol. 2016 Jun 24;90(14):6216-6223. doi: 10.1128/JVI.00121-16. Print 2016 Jul 15. J Virol. 2016. PMID: 27122579 Free PMC article.
-
The N Terminus of Human Cytomegalovirus Glycoprotein O Is Important for Binding to the Cellular Receptor PDGFRα.J Virol. 2019 May 15;93(11):e00138-19. doi: 10.1128/JVI.00138-19. Print 2019 Jun 1. J Virol. 2019. PMID: 30894468 Free PMC article.
-
Seminal plasma and semen amyloids enhance cytomegalovirus infection in cell culture.J Virol. 2013 Dec;87(23):12583-91. doi: 10.1128/JVI.02083-13. Epub 2013 Sep 11. J Virol. 2013. PMID: 24027327 Free PMC article.
-
Human cytomegalovirus tropism for endothelial/epithelial cells: scientific background and clinical implications.Rev Med Virol. 2010 May;20(3):136-55. doi: 10.1002/rmv.645. Rev Med Virol. 2010. PMID: 20084641 Review.
-
Principles for studying in vivo attenuation of virus mutants: defining the role of the cytomegalovirus gH/gL/gO complex as a paradigm.Med Microbiol Immunol. 2015 Jun;204(3):295-305. doi: 10.1007/s00430-015-0405-2. Epub 2015 Mar 18. Med Microbiol Immunol. 2015. PMID: 25782576 Review.
Cited by
-
Potent Restriction of Sexual Zika Virus Infection by the Lipid Fraction of Extracellular Vesicles in Semen.Front Microbiol. 2020 Sep 29;11:574054. doi: 10.3389/fmicb.2020.574054. eCollection 2020. Front Microbiol. 2020. PMID: 33133043 Free PMC article.
-
Editorial: Immune barrier, viral sanctuaries, and sexual transmission in the male reproductive system.Front Immunol. 2023 Feb 7;14:1139520. doi: 10.3389/fimmu.2023.1139520. eCollection 2023. Front Immunol. 2023. PMID: 36825015 Free PMC article. No abstract available.
-
Current status of the COVID-19 and male reproduction: A review of the literature.Andrology. 2021 Jul;9(4):1066-1075. doi: 10.1111/andr.13037. Epub 2021 Jun 10. Andrology. 2021. PMID: 33998143 Free PMC article. Review.
-
The Bovine Seminal Plasma Protein PDC-109 Possesses Pan-Antiviral Activity.Viruses. 2022 Sep 13;14(9):2031. doi: 10.3390/v14092031. Viruses. 2022. PMID: 36146836 Free PMC article.
-
Cytomegalovirus (CMV) Pneumonitis: Cell Tropism, Inflammation, and Immunity.Int J Mol Sci. 2019 Aug 8;20(16):3865. doi: 10.3390/ijms20163865. Int J Mol Sci. 2019. PMID: 31398860 Free PMC article. Review.
References
-
- Rawlinson WD, Boppana SB, Fowler KB, Kimberlin DW, Lazzarotto T, Alain S, Daly K, Doutr S, Gibson L, Giles ML, Greenlee J, Hamilton ST, Harrison GJ, Hui L, Jones CA, Palasanthiran P, Schleiss MR, Shand AW, van Zuylen WJ. 2017. Congenital cytomegalovirus infection in pregnancy and the neonate: consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect Dis 17:e177–e188. doi:10.1016/S1473-3099(17)30143-3. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
