

Review
doi: 10.3348/kjr.2018.0040.
Epub 2018 Dec 27.
What Is New in the 2017 World Health Organization Classification and 8th American Joint Committee on Cancer Staging System for Pancreatic Neuroendocrine Neoplasms?
Affiliations
- PMID: 30627018
- PMCID: PMC6315069
- DOI: 10.3348/kjr.2018.0040
Item in Clipboard
Review
What Is New in the 2017 World Health Organization Classification and 8th American Joint Committee on Cancer Staging System for Pancreatic Neuroendocrine Neoplasms?
Korean J Radiol.
2019 Jan.
Abstract
The diagnosis and management of pancreatic neuroendocrine neoplasms (NENs) have evolved significantly in recent years. There are several diagnostic and therapeutic challenges and controversies regarding the management of these lesions. In this review, we focus on the recent significant changes and controversial issues regarding the diagnosis and management of NENs and discuss the role of imaging in the multidisciplinary team approach.
Keywords: Management; Multidisciplinary; NET; Neuroendocrine tumor; Pancreas; Staging.
Conflict of interest statement
Conflicts of Interest: The authors have no financial conflicts of interest.
Figures
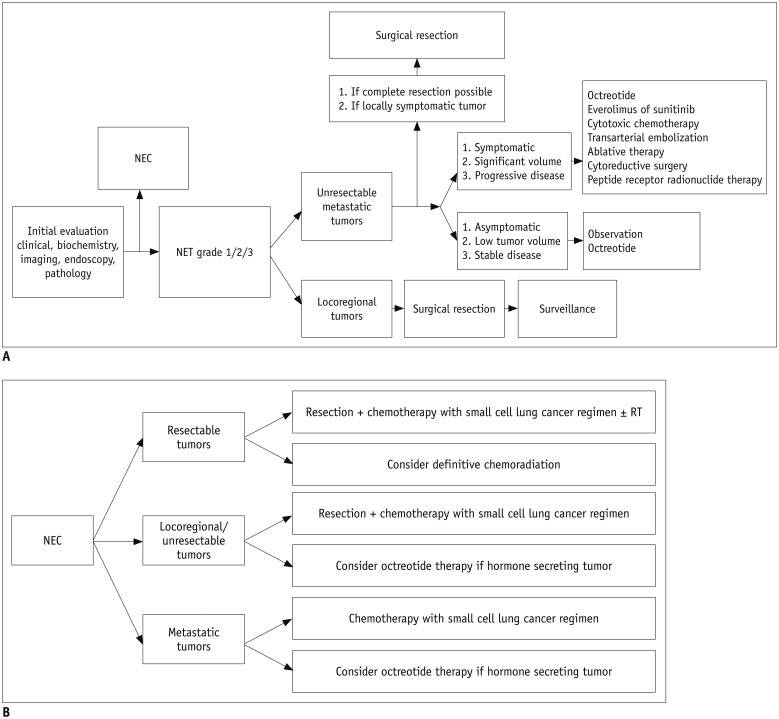
Revised from 2017 National Comprehensive Cancer Network guidelines. A. NET. B. NEC. NEC = neuroendocrine carcinomas, NENs = neuroendocrine neoplasms, NET = neuroendocrine tumor, RT = radiation therapy

A. Low-grade NET is generally small-sized and has well-defined margins on imaging (arrow). B. Higher-grade NET is likely to be larger or more frequently show necrotic change (arrow). C. NEC shows less enhancement than NET, and presents as iso-enhancing or hypoenhancing mass in pancreas. Margin of NEC may be less well demarcated than that of NET (arrow).
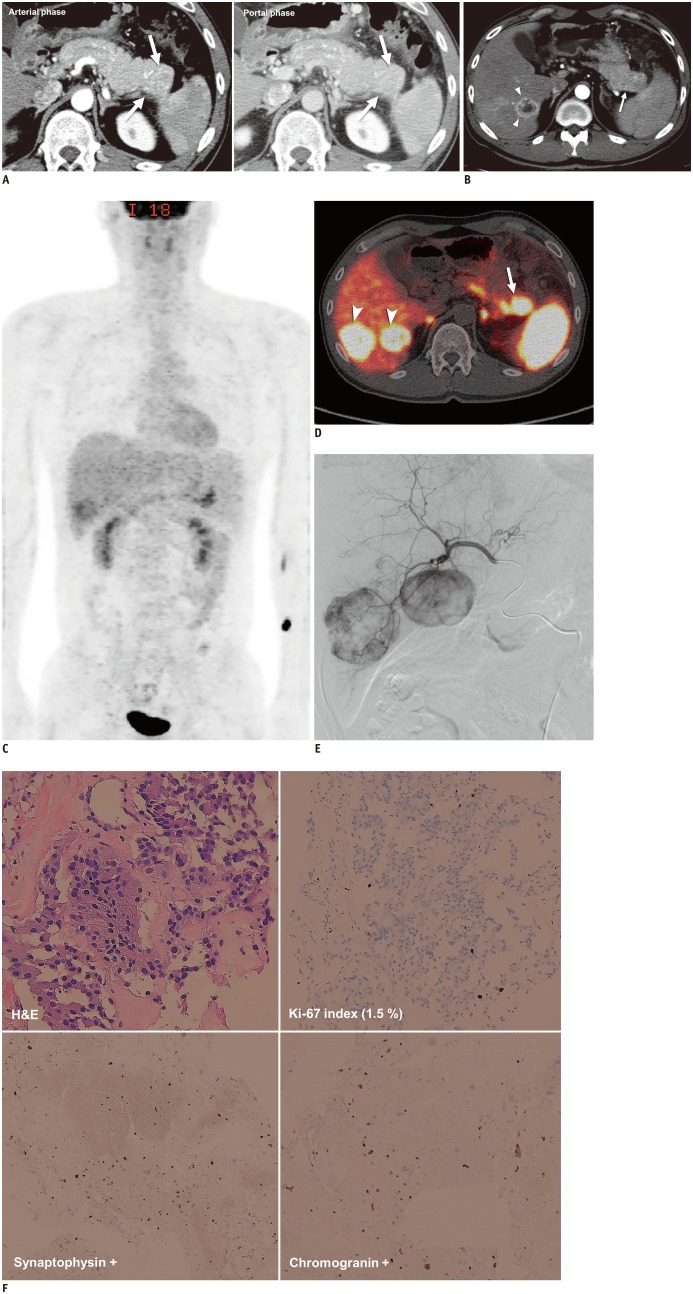
A. 2.9-cm, arterial enhancing hypervascular mass in tail of pancreas was found on initial contrast-enhanced CT (arrows). B. After seven years, hypervascular mass in tail of pancreas had increased in size (arrow) and there was new hypervascular mass in liver (arrowheads), suggestive of hepatic metastasis. Fluid collection and peripancreatic infiltration were also present because of secondary pancreatitis. C. On 18F-FDG PET/CT, tumors showed negative or weak uptake. D. PET/CT with 68gallium-labeled somatostatin analog revealed 3.3-cm mass with markedly increased uptake (maximum standard uptake value, 40.6) in tail of pancreas (arrow), other foci in body of pancreas, and additional hepatic masses (arrowheads) with increased uptake, suggesting multifocal NET with overexpression of somatostatin receptor. Physiologic uptake was seen in both adrenal glands. E. Patient underwent transarterial embolization for management of hepatic metastases and arteriography showed hypervascular mass in right portion of liver. CT = computed tomography, FDG = fluorodeoxyglucose, PET = positron-emission tomography F. On histologic specimens (× 100) obtained during liver biopsy, tumor appeared to have relatively uniform and round nuclei with abundant cytoplasmic granules on H&E staining, low Ki-67 index (1.5%), and diffuse positivity on synaptophysin and chromogranin staining. These imaging and histologic findings suggested morphologically well-differentiated NET. H&E = hematoxylin and eosin
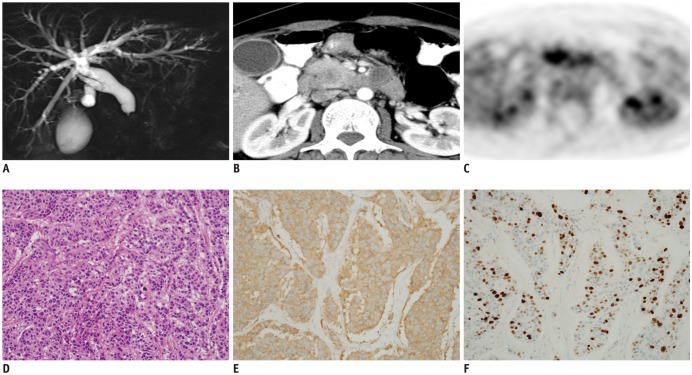
This patient was referred to our hospital with tentative diagnosis of ductal carcinoma of pancreas. A. Magnetic resonance cholangiopancreatography showed abrupt tapering of intrapancreatic common bile duct with diffuse upstream dilatation. B. Contrast-enhanced CT showed 2.5-cm, relatively well-defined, low attenuating solid mass in head of pancreas. C. Tumor showed high FDG avidity on FDG-PET. Imaging reports suggested possibility of NEC as well as ductal adenocarcinoma of pancreas, indicating need for biopsy. D. H&E staining (× 40) revealed small, round, blue cells in tumor. Immunohistochemistry specimens (× 40) showed positivity on synaptophysin (E) and Ki-67 (F) staining with Ki-67 proliferation index of 70%. These findings confirmed diagnosis of NEC.

A. Intraductal growth in 42-year-old woman. Axial contrast-enhanced CT scan shows large mass (arrow on left) with intraductal growth causing diffuse dilatation of bile duct upstream (arrows on right). First differential diagnosis was invasive cancer arising from intraductal papillary mucinous neoplasm. However, lesion was confirmed to be grade 3 NEC after surgical resection. B. Cystic change in 48-year-old man. Axial contrast-enhanced CT image shows 5.6-cm cystic lesion with relatively thick wall in tail of pancreas. Preoperative imaging diagnosis was pseudocyst or cystic neoplasm of pancreas. However, surgical specimen confirmed that lesion was grade 1 NET with cystic change. C. Vascular invasion with tumor thrombus in 29-year-old man. Axial contrast-enhanced CT image shows large heterogeneous attenuating mass involving body and tail of pancreas and left para-aortic area (arrowhead). Vascular invasion is apparent and there is tumor thrombus extending into splenoportal confluence (arrow). Biopsy confirmed diagnosis of grade 3 NEC.
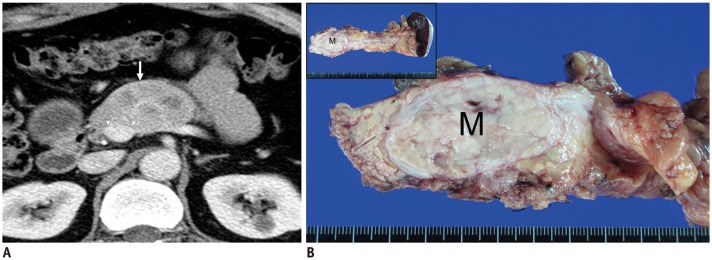
A. Contrast-enhanced axial CT scan in 48-year-old man with NET in body of pancreas. Scan shows 5-cm mass (arrow) distortion of contour of main portal vein because of circumferential contact between tumor and portal vein of more than 180 degrees (arrowheads). These CT findings may suggest vessel invasion and indicate unresectability. B. Surgical specimen. Exploratory surgery in this patient confirmed that tumor was resectable in that main portal vein was severely compressed by tumor but without apparent vessel invasion. Therefore, distal pancreatectomy and splenectomy were performed. Gross specimen showed well-defined, ovoid soft-tissue mass (M) in body of pancreas but without vessel invasion.
References
-
- Singhi AD, Klimstra DS. Well-differentiated pancreatic neuroendocrine tumours (PanNETs) and poorly differentiated pancreatic neuroendocrine carcinomas (PanNECs): concepts, issues and a practical diagnostic approach to high-grade (G3) cases. Histopathology. 2018;72:168–177. - PubMed
-
- Lawrence B, Gustafsson BI, Chan A, Svejda B, Kidd M, Modlin IM. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin North Am. 2011;40:1–18. - PubMed
-
- Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 4th ed. Lyon: International Agency for Research on Cancer; 2010.
-
- Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010;39:707–712. - PubMed
-
- Edge S, Byrd DR, Compton CC, Fritz AG, Greene F, Trotti A. AJCC cancer staging manual. 7th ed. New York, NY: Springer; 2010. pp. 181–190.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
