

Four-Dimensional Thoracic CT in Free-Breathing Children
- PMID: 30627021
- PMCID: PMC6315071
- DOI: 10.3348/kjr.2018.0325
Four-Dimensional Thoracic CT in Free-Breathing Children
Abstract
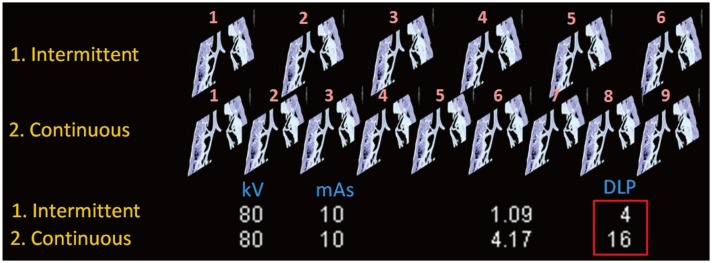
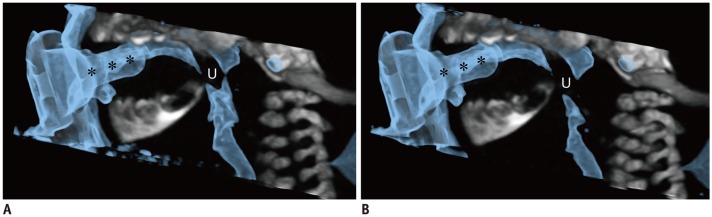
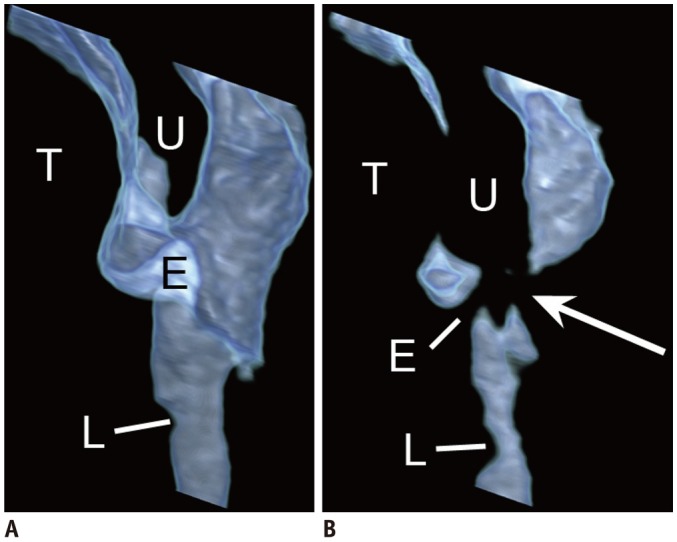
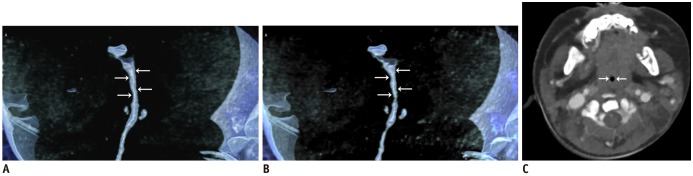
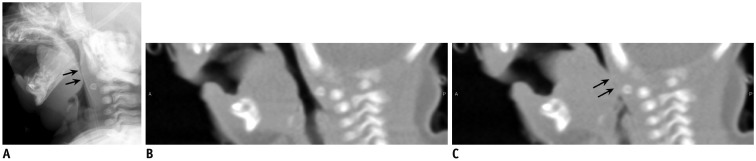
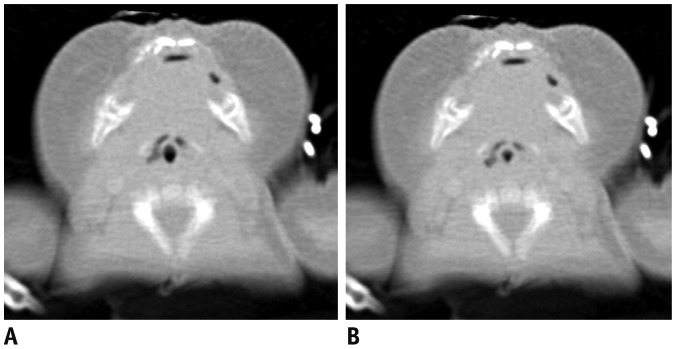
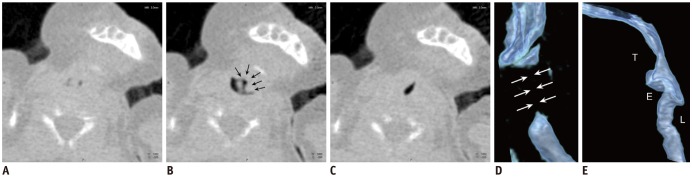
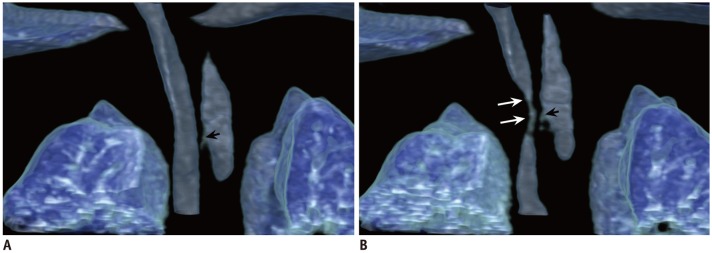
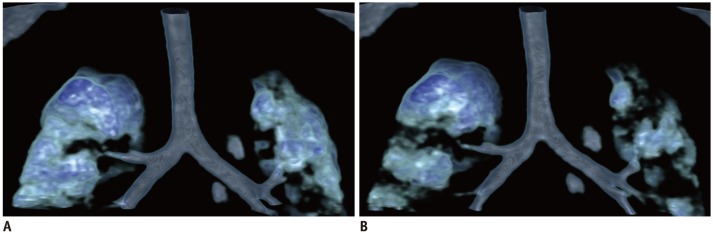
In pediatric thoracic CT, respiratory motion is generally treated as a motion artifact degrading the image quality. Conversely, respiratory motion in the thorax can be used to answer important clinical questions, that cannot be assessed adequately via conventional static thoracic CT, by utilizing four-dimensional (4D) CT. However, clinical experiences of 4D thoracic CT are quite limited. In order to use 4D thoracic CT properly, imagers should understand imaging techniques, radiation dose optimization methods, and normal as well as typical abnormal imaging appearances. In this article, the imaging techniques of pediatric thoracic 4D CT are reviewed with an emphasis on radiation dose. In addition, several clinical applications of pediatric 4D thoracic CT are addressed in various thoracic functional abnormalities, including upper airway obstruction, tracheobronchomalacia, pulmonary air trapping, abnormal diaphragmatic motion, and tumor invasion. One may further explore the clinical usefulness of 4D thoracic CT in free-breathing children, which can enrich one's clinical practice.
Keywords: 4D CT; Air trapping; Airway; CT imaging techniques; Chest CT; Child; Diaphragm motion; Lung densitometry; Tracheobronchomalacia; Tumor invasion.
Conflict of interest statement
Conflicts of Interest: The author has no financial conflicts of interest.
Figures
References
-
- Lee EY, Mason KP, Zurakowski D, Waltz DA, Ralph A, Riaz F, et al. MDCT assessment of tracheomalacia in symptomatic infants with mediastinal aortic vascular anomalies: preliminary technical experience. Pediatr Radiol. 2008;38:82–88. - PubMed
-
- Long FR, Castile RG, Brody AS, Hogan MJ, Flucke RL, Filbrun DA, et al. Lungs in infants and young children: improved thin-section CT with a noninvasive controlled-ventilation technique--initial experience. Radiology. 1999;212:588–593. - PubMed
-
- Goo HW. Combined prospectively electrocardiography- and respiratory-triggered sequential cardiac computed tomography in free-breathing children: success rate and image quality. Pediatr Radiol. 2018;48:923–931. - PubMed
-
- Lin L, Bivard A, Krishnamurthy V, Levi CR, Parsons MW. Whole-brain CT perfusion to quantify acute ischemic penumbra and core. Radiology. 2016;279:876–887. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
