

Change in Survival in Metastatic Breast Cancer with Treatment Advances: Meta-Analysis and Systematic Review
- PMID: 30627694
- PMCID: PMC6305243
- DOI: 10.1093/jncics/pky062
Change in Survival in Metastatic Breast Cancer with Treatment Advances: Meta-Analysis and Systematic Review
Abstract
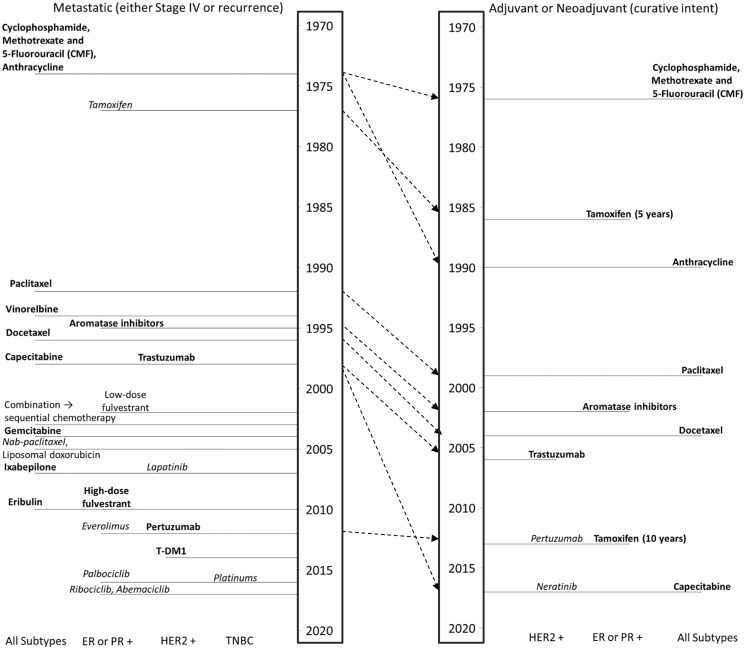
Background: Metastatic breast cancer (MBC) treatment has changed substantially over time, but we do not know whether survival post-metastasis has improved at the population level.
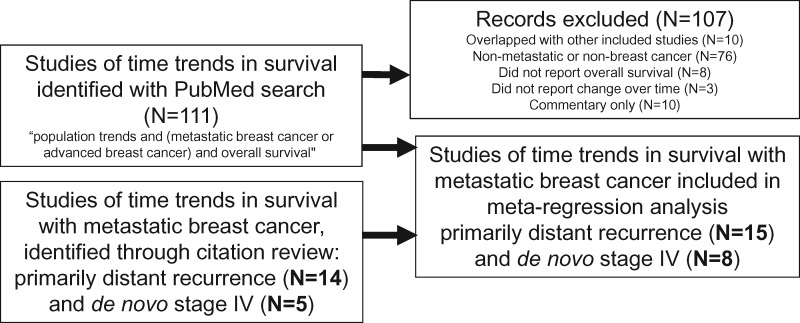
Methods: We searched for studies of MBC patients that reported survival after metastasis in at least two time periods between 1970 and the present. We used meta-regression models to test for survival improvement over time in four disease groups: recurrent, recurrent estrogen (ER)-positive, recurrent ER-negative, and de novo stage IV. We performed sensitivity analyses based on bias in some studies that could lead earlier cohorts to include more aggressive cancers.
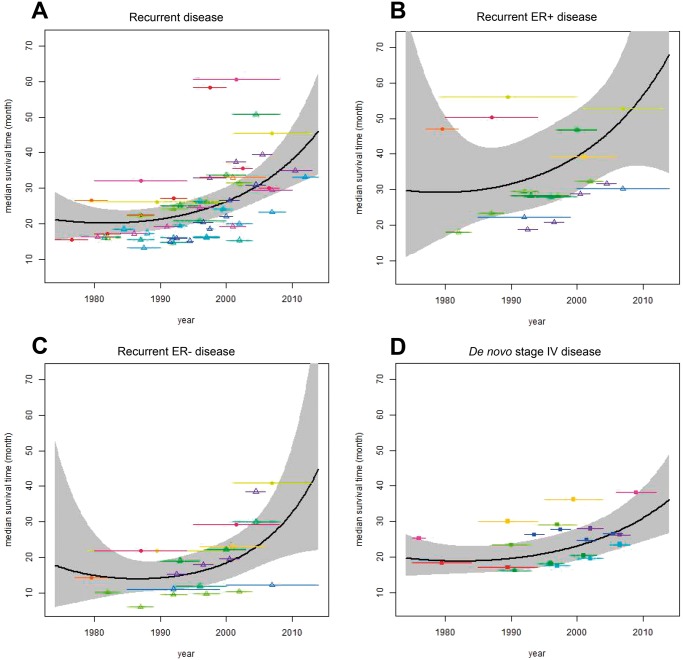
Results: There were 15 studies of recurrent MBC (N = 18 678 patients; 3073 ER-positive and 1239 ER-negative); meta-regression showed no survival improvement among patients recurring between 1980 and 1990, but median survival increased from 21 (95% confidence interval [CI] = 18 to 25) months to 38 (95% CI = 31 to 47) months from 1990 to 2010. For ER-positive MBC patients, median survival increased during 1990-2010 from 32 (95% CI = 23 to 43) to 57 (95% CI = 37 to 87) months, and for ER-negative MBC patients from 14 (95% CI = 11 to 19) to 33 (95% CI = 21 to 51) months. Among eight studies (N = 35 831) of de novo stage IV MBC, median survival increased during 1990-2010 from 20 (95% CI = 16 to 24) to 31 (95% CI = 24 to 39) months. Results did not change in sensitivity analyses.
Conclusion: By bridging studies over time, we demonstrated improvements in survival for recurrent and de novo stage IV MBC overall and across ER-defined subtypes since 1990. These results can inform patient-doctor discussions about MBC prognosis and therapy.
Figures
References
-
- Torre LA, Islami F, Siegel RL, et al. Global cancer in women: burden and trends. Cancer Epidemiol Biomarkers Prev. 2017;264:444–457. - PubMed
-
- Siegel RL, Miller KD, Jemal A.. Cancer statistics, 2017. CA Cancer J Clin. 2017;671:7–30. - PubMed
-
- Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;35317:1784–1792. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical