

Choroideremia: from genetic and clinical phenotyping to gene therapy and future treatments
- PMID: 30627697
- PMCID: PMC6311551
- DOI: 10.1177/2515841418817490
Choroideremia: from genetic and clinical phenotyping to gene therapy and future treatments
Abstract
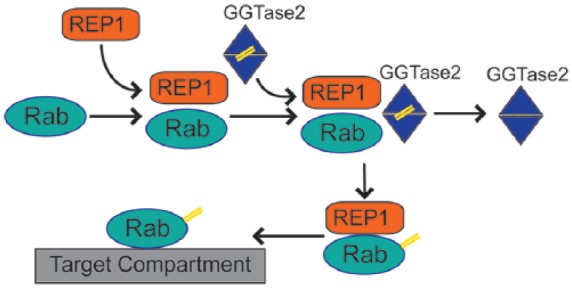
Choroideremia is an X-linked inherited chorioretinal dystrophy leading to blindness by late adulthood. Choroideremia is caused by mutations in the CHM gene which encodes Rab escort protein 1 (REP1), an ubiquitously expressed protein involved in intracellular trafficking and prenylation activity. The exact site of pathogenesis remains unclear but results in degeneration of the photoreceptors, retinal pigment epithelium and choroid. Animal and stem cell models have been used to study the molecular defects in choroideremia and test effectiveness of treatment interventions. Natural history studies of choroideremia have provided additional insight into the clinical phenotype of the condition and prepared the way for clinical trials aiming to investigate the safety and efficacy of suitable therapies. In this review, we provide a summary of the current knowledge on the genetics, pathophysiology, clinical features and therapeutic strategies that might become available for choroideremia in the future, including gene therapy, stem cell treatment and small-molecule drugs with nonsense suppression action.
Keywords: REP1; choroideremia; gene therapy; nonsense suppression therapy; retinal dystrophy; stem cells.
Conflict of interest statement
Conflict of interest statement: The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures
References
-
- MacDonald IM, Sereda C, McTaggart K, et al. Choroideremia gene testing. Expert Rev Mol Diagn 2004; 4: 478–484. - PubMed
-
- U.S. National Library of Medicine, National Institutes of Health, Department of Health & Human Services. Choroideremia, https://ghr.nlm.nih.gov/condition/choroideremia#statistics (accessed 2 January 2018).
-
- Sankila EM, Chapelle ADLA, Karna J, et al. Choroideremia: close linkage to DXYS1 and DXYS12 demonstrated by segregation analysis and historical-genealogical evidence. Clin Genet 1987; 31: 315–322. - PubMed
-
- Sankila EM, Tolvanen R, van den Hurk JAJM, et al. Aberrant splicing of the CHM gene is a significant cause of choroideremia. Nat Genet 1992; 1: 109–113. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
