

Persistence and effectiveness of nonbiologic systemic therapies for moderate-to-severe psoriasis in adults: a systematic review
- PMID: 30628069
- PMCID: PMC6766878
- DOI: 10.1111/bjd.17625
Persistence and effectiveness of nonbiologic systemic therapies for moderate-to-severe psoriasis in adults: a systematic review
Abstract
Background: The persistence and effectiveness of systemic therapies for moderate-to-severe psoriasis in current clinical practice are poorly characterized.
Objectives: To systematically review observational studies investigating the persistence and effectiveness of acitretin, ciclosporin, fumaric acid esters (FAE) and methotrexate, involving at least 100 adult patients with moderate-to-severe psoriasis, exposed to therapy for ≥ 3 months.
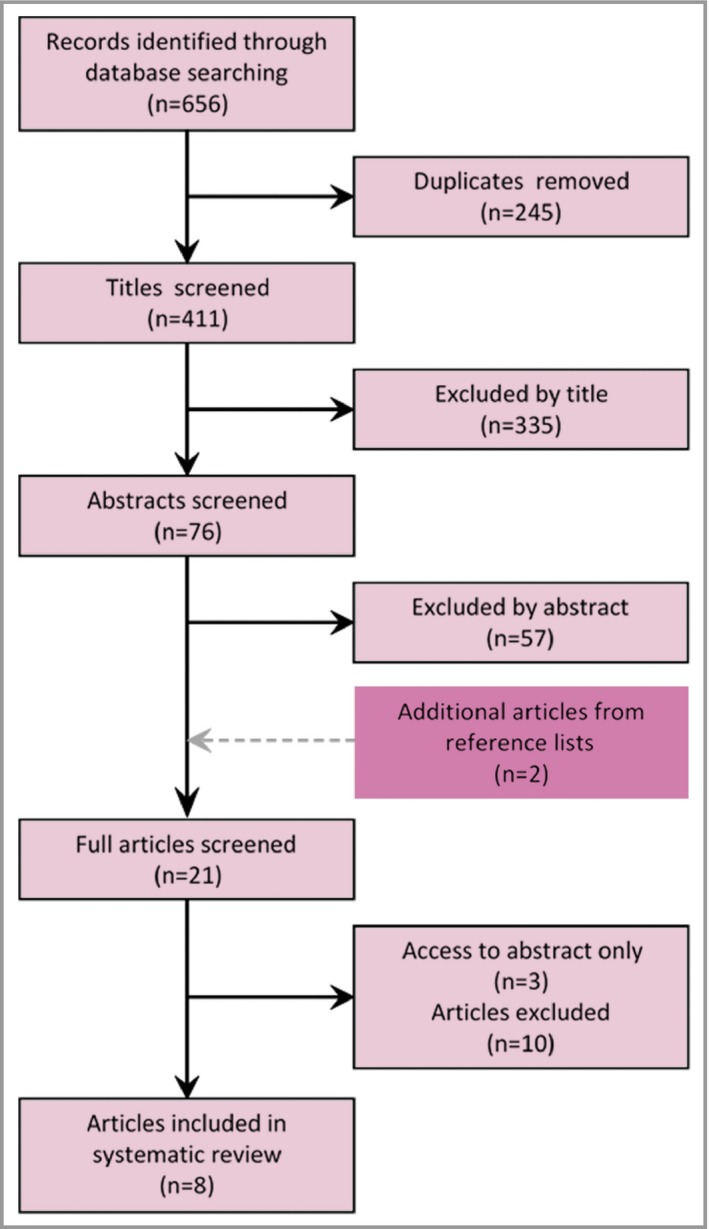
Methods: MEDLINE, Embase, the Cochrane Library and PubMed were searched from 1 January 2007 to 1 November 2017 for observational studies reporting on persistence (therapy duration or the proportion of patients discontinuing therapy during follow-up) or effectiveness [improvements in Psoriasis Area and Severity Index (PASI) or Physician's Global Assessment (PGA)]. This review was registered with PROSPERO, number CRD42018099771.
Results: Of 411 identified studies, eight involving 4624 patients with psoriasis were included. Variations in the definitions and analyses of persistence and effectiveness outcomes prevented a meta-analysis from being conducted. One prospective multicentre study reported drug survival probabilities of 23% (ciclosporin), 42% (acitretin) and 50% (methotrexate) at 1 year. Effectiveness outcomes were not reported for either acitretin or ciclosporin. The persistence and effectiveness of FAE and methotrexate were better characterized, but mean discontinuation times ranged from 28 to 50 months for FAE and 7·7 to 22·3 months for methotrexate. At 12 months of follow-up, three studies reported that 76% (FAE), 53% (methotrexate) and 59% (methotrexate) of patients achieved ≥ 75% reduction in PASI, and one reported that 76% of FAE-exposed patients achieved a markedly improved or clear PGA.
Conclusions: The comparative persistence and effectiveness of acitretin, ciclosporin, FAE and methotrexate in real-world clinical practice in the past decade cannot be well described due to the inconsistency of the methods used.
© 2019 The Authors. British Journal of Dermatology published by John Wiley & Sons Ltd on behalf of British Association of Dermatologists.
Conflict of interest statement
K.J.M. has received honoraria from Eli Lilly and Janssen. K.M. has received honoraria from Eli Lilly. D.M.A. has received research grants from AbbVie, Almirall, Celgene, Eli Lilly, Novartis, UCB and the LEO Foundation. C.E.K. has acted as a consultant and/or speaker for and/or received research grants from AbbVie, Almirall, Celgene, Eli Lilly, Pfizer, LEO Pharma, Novartis, Janssen Cilag, Medac and UCB Pharma. N.J.R. reports research grants from AstraZeneca and Stiefel GSK; and other income to Newcastle University from Almirall, Amgen, Janssen and Novartis for lectures or attendance at advisory boards. C.H.S. has received research funding from AbbVie, GSK, Pfizer, Novartis, Regeneron and Roche. R.B.W. has acted as a consultant and/or speaker for and/or received research grants from AbbVie, Amgen, Almirall, Celgene, Eli Lilly, Pfizer, LEO Pharma, Novartis, Janssen Cilag, Medac, UCB Pharma and Xenoport. C.E.M.G. has received honoraria and/or research grants from AbbVie, Almirall, Amgen, Bristol‐Myers Squibb, Celgene, Galderma, LEO Pharma, Eli Lilly, GSK‐Stiefel, Janssen Cilag, MSD, Novartis, Pfizer, Sandoz and UCB Pharma. S.W., Z.Z.N.Y., Z.K.J.L., C.M.O. and N.W. declare no conflicts of interest.
Figures
Comment in
-
Effectiveness of classic drugs in psoriasis: still alive.Br J Dermatol. 2019 Aug;181(2):237. doi: 10.1111/bjd.17876. Epub 2019 Jun 28. Br J Dermatol. 2019. PMID: 31250919 No abstract available.
References
-
- Dubertret L, Mrowietz U, Ranki A et al European patient perspectives on the impact of psoriasis: the EUROPSO patient membership survey. Br J Dermatol 2006; 155:729–36. - PubMed
-
- Strober BE, Siu K, Menon K. Conventional systemic agents for psoriasis. A systematic review. J Rheumatol 2006; 33:1442–6. - PubMed
-
- National Institute for Health and Care Excellence . Psoriasis: assessment and management. Clinical guideline CG153. Available at: https://www.nice.org.uk/guidance/cg153 (last accessed 14 February 2019). - PubMed
-
- Garcia‐Doval I, Carretero G, Vanaclocha F et al Risk of serious adverse events associated with biologic and nonbiologic psoriasis systemic therapy: patients ineligible versus eligible for randomized controlled trials. Arch Dermatol 2012; 148:463–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
