

Assessment of a Watch-and-Wait Strategy for Rectal Cancer in Patients With a Complete Response After Neoadjuvant Therapy
- PMID: 30629084
- PMCID: PMC6459120
- DOI: 10.1001/jamaoncol.2018.5896
Assessment of a Watch-and-Wait Strategy for Rectal Cancer in Patients With a Complete Response After Neoadjuvant Therapy
Abstract
Importance: The watch-and-wait (WW) strategy aims to spare patients with rectal cancer unnecessary resection.
Objective: To analyze the outcomes of WW among patients with rectal cancer who had a clinical complete response to neoadjuvant therapy.
Design, setting, and participants: This retrospective case series analysis conducted at a comprehensive cancer center in New York included patients who received a diagnosis of rectal adenocarcinoma between January 1, 2006, and January 31, 2015. The median follow-up was 43 months. Data analyses were conducted from June 1, 2016, to October 1, 2018.
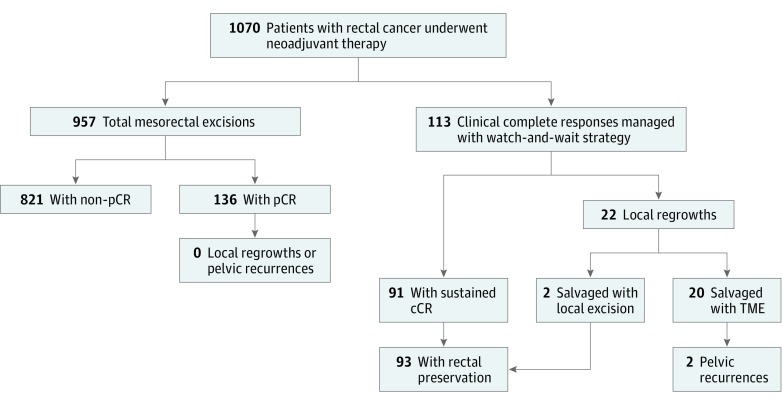
Exposures: Patients had a clinical complete response after completing neoadjuvant therapy and agreed to a WW strategy of active surveillance and possible salvage surgery (n = 113), or patients underwent total mesorectal excision and were found to have a pathologic complete response (pCR) at resection (n = 136).
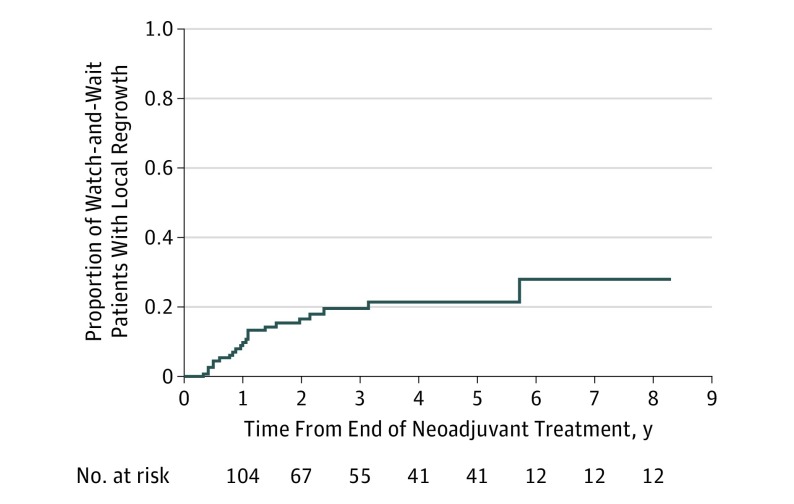
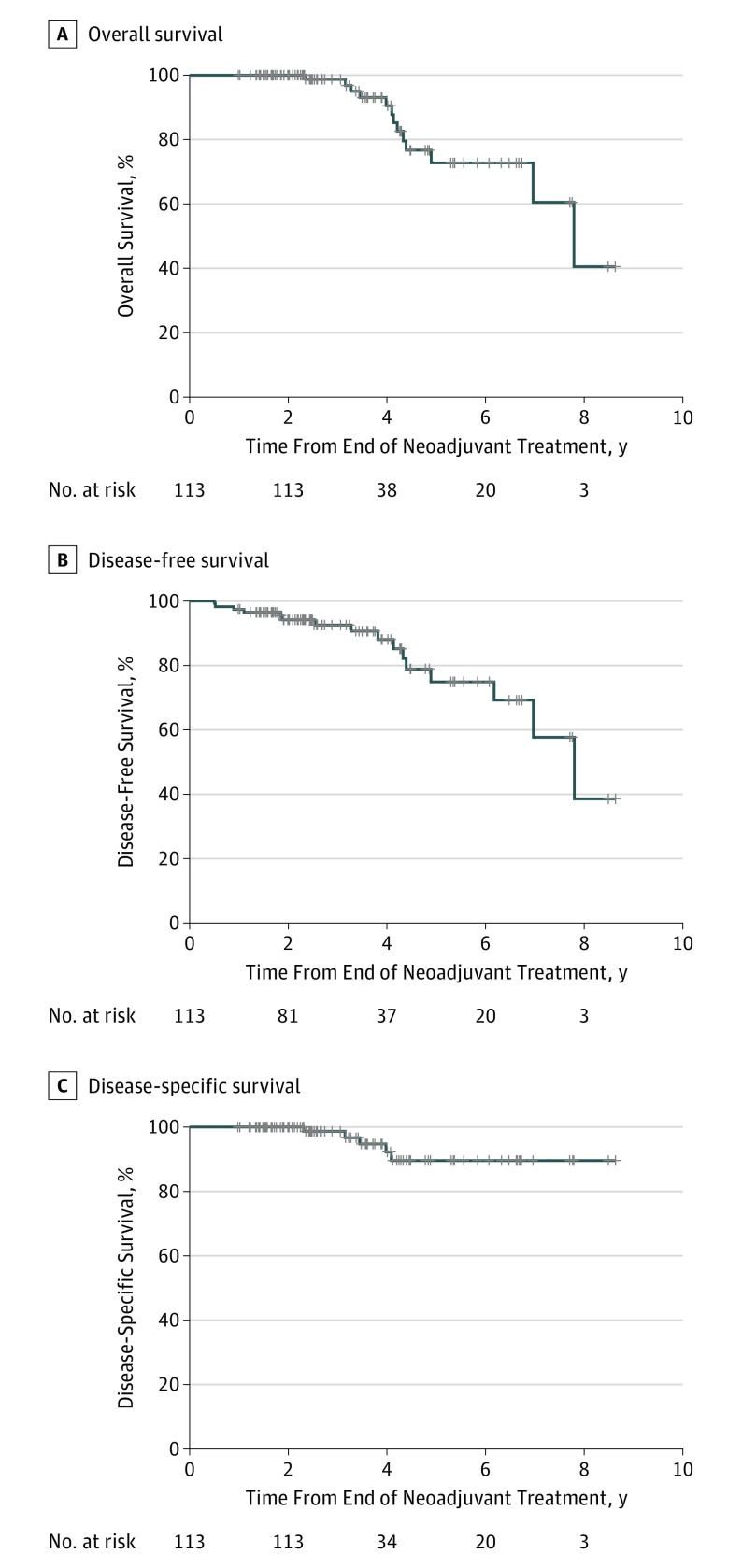
Main outcomes and measures: Kaplan-Meier estimates were used for analyses of local regrowth and 5-year rates of overall survival, disease-free survival, and disease-specific survival.
Results: Compared with the 136 patients in the pCR group, the 113 patients in the WW group were older (median [range], 67.2 [32.1-90.9] vs 57.3 [25.0-87.9] years, P < .001) with cancers closer to the anal verge (median [range] height from anal verge, 5.5 [0.0-15.0] vs 7.0 [0.0-13.0] cm). All 22 local regrowths in the WW group were detected on routine surveillance and treated by salvage surgery (20 total mesorectal excisions plus 2 transanal excisions). Pelvic control after salvage surgery was maintained in 20 of 22 patients (91%). No pelvic recurrences occurred in the pCR group. Rectal preservation was achieved in 93 of 113 patients (82%) in the WW group (91 patients with no local regrowths plus 2 patients with local regrowths salvaged with transanal excision). At 5 years, overall survival was 73% (95% CI, 60%-89%) in the WW group and 94% (95% CI, 90%-99%) in the pCR group; disease-free survival was 75% (95% CI, 62%-90%) in the WW group and 92% (95% CI, 87%-98%) in the pCR group; and disease-specific survival was 90% (95% CI, 81%-99%) in the WW group and 98% (95% CI, 95%-100%) in the pCR group. A higher rate of distant metastasis was observed among patients in the WW group who had local regrowth vs those who did not have local regrowth (36% vs 1%, P < .001).
Conclusions and relevance: A WW strategy for select rectal cancer patients who had a clinical complete response after neoadjuvant therapy resulted in excellent rectal preservation and pelvic tumor control; however, in the WW group, worse survival was noted along with a higher incidence of distant progression in patients with local regrowth vs those without local regrowth.
Conflict of interest statement
Figures
Comment in
-
Is Watch-and-Wait Ready for Prime Time?: It Depends on Priming of the Multidisciplinary Care Team.JAMA Oncol. 2019 Apr 1;5(4):e185895. doi: 10.1001/jamaoncol.2018.5895. Epub 2019 Apr 11. JAMA Oncol. 2019. PMID: 30629098 No abstract available.
-
Gastrointestinal Cancers: Fine-Tuning the Management of Rectal, Esophageal, and Pancreas Cancers.Int J Radiat Oncol Biol Phys. 2019 Sep 1;105(1):1-10. doi: 10.1016/j.ijrobp.2019.04.037. Int J Radiat Oncol Biol Phys. 2019. PMID: 31422802 Free PMC article. No abstract available.
References
-
- Chow OS, Smith JJ, Gollub MJ, Garcia-Aguilar J. Can we predict response and/or resistance to neoadjuvant chemoradiotherapy in patients with rectal cancer? Curr Colorectal Cancer Rep. 2014;10(2):164-172. doi:10.1007/s11888-014-0210-0 - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
