

Validation of the extended thrombolysis in cerebral infarction score in a real world cohort
- PMID: 30629664
- PMCID: PMC6328192
- DOI: 10.1371/journal.pone.0210334
Validation of the extended thrombolysis in cerebral infarction score in a real world cohort
Abstract
Background: A thrombolysis in cerebral infarction (TICI) score of 2b is defined as a good recanalization result although the reperfusion may only cover 50% of the affected territory. An additional mTICI2c category was introduced to further differentiate between mTICI scores. Despite the new mTICI2c category, mTICI2b still covers a range of 50-90% reperfusion which might be too imprecise to predict neurological improvement after therapy.
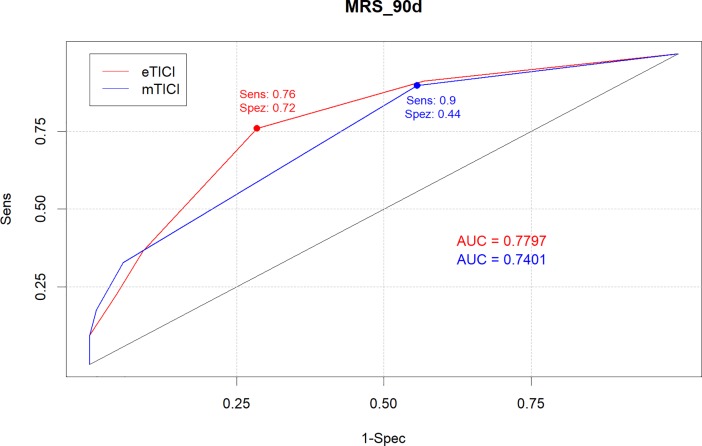
Aim: To compare the 7-point "expanded TICI" (eTICI) scale with the traditional mTICI in regard to predict functional independence at 90 days.
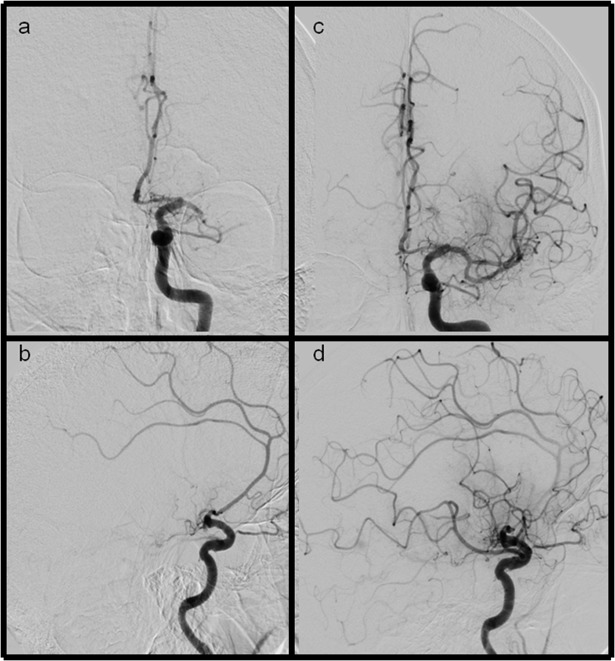
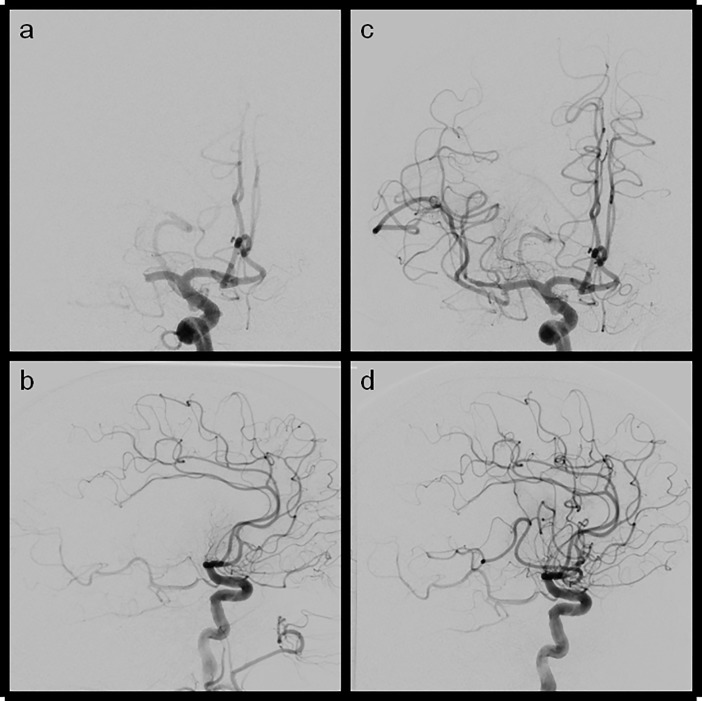
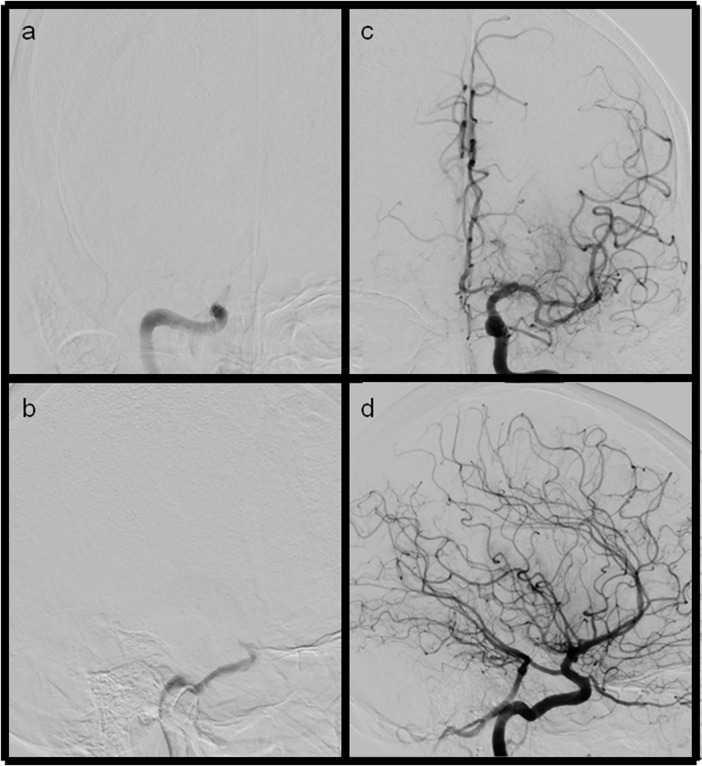
Methods: Retrospective review of 225 patients with large artery occlusion. Angiograms were graded by 2 readers according the 7-point eTICI score (0% = eTICI0; reduced clot = eTICI1; 1-49% = eTICI2a, 50-66% = eTICI2b50; 67-89% = eTICI2b67, 90-99% = eTICI2c and complete reperfusion = eTICI3) and the conventional mTICI score. The ability of e- and mTICI to predict favorable outcome at 90days was compared.
Results: Given the ROC analysis eTICI was the better predictor of favorable outcome (p-value 0.047). Additionally, eTICI scores 2b50, 2b67 and 2c (former mTICI2b) were significantly superior at predicting the probability of a favorable outcome at 90 days after endovascular therapy with a p-value of 0.033 (probabilities of 17% for mTICI2b50, 24% for mTICI2b67 and 54% for mTICI2c vs. 36% for mTICI2b).
Conclusions: The 7-point eTICI allows for a more accurate outcome prediction compared to the mTICI score because it refines the broad range of former mTICI2b results.
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies: All: none regarding the content of the manuscript. DB is consultant for Phenox. Minor speaking honorary and travel grants were received by MNP and DB from Siemens, Phenox, Penumbra, Acandis and Stryker. All other authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723–31. Epub 2016/02/24. 10.1016/S0140-6736(16)00163-X . - DOI - PubMed
-
- Rozeman AD, Wermer MJ, Vos JA, Lycklama a Nijeholt GJ, Beumer D, Berkhemer OA, et al. Evolution of Intra-arterial Therapy for Acute Ischemic Stroke in The Netherlands: MR CLEAN Pretrial Experience. Journal of stroke and cerebrovascular diseases: the official journal of National Stroke Association. 2016;25(1):115–21. Epub 2015/10/13. 10.1016/j.jstrokecerebrovasdis.2015.09.002 . - DOI - PubMed
-
- Zaidat OO, Yoo AJ, Khatri P, Tomsick TA, von Kummer R, Saver JL, et al. Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke: A Consensus Statement. Stroke; a journal of cerebral circulation. 2013;44(9):2650–63. Epub 2013/08/08. 10.1161/strokeaha.113.001972 . - DOI - PMC - PubMed
-
- Jayaraman MV, Grossberg JA, Meisel KM, Shaikhouni A, Silver B. The clinical and radiographic importance of distinguishing partial from near-complete reperfusion following intra-arterial stroke therapy. AJNR American journal of neuroradiology. 2013;34(1):135–9. Epub 2012/07/28. 10.3174/ajnr.A3278 . - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
