

Failure of bumetanide to improve outcome after intracerebral hemorrhage in rat
- PMID: 30629699
- PMCID: PMC6328169
- DOI: 10.1371/journal.pone.0210660
Failure of bumetanide to improve outcome after intracerebral hemorrhage in rat
Abstract
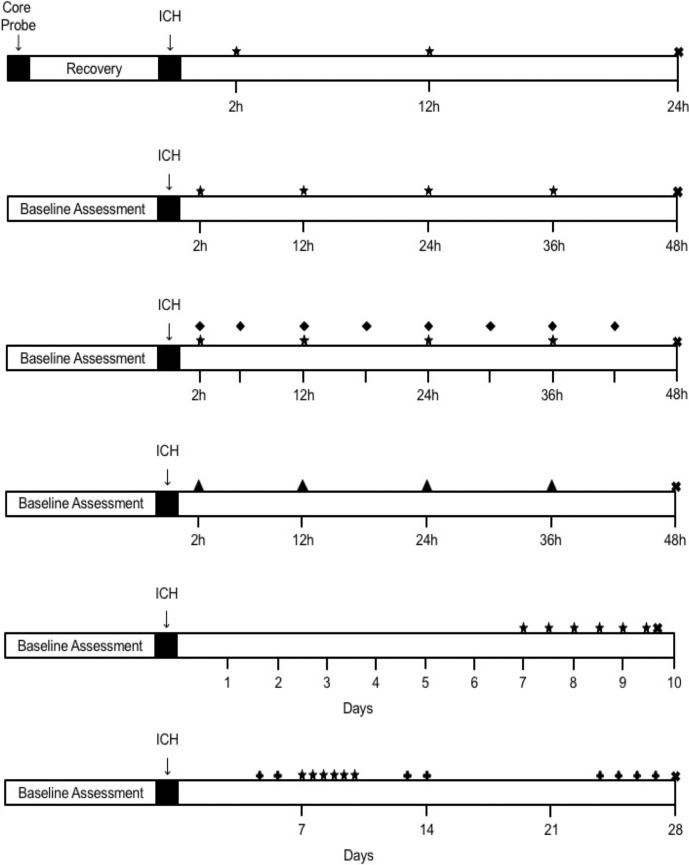
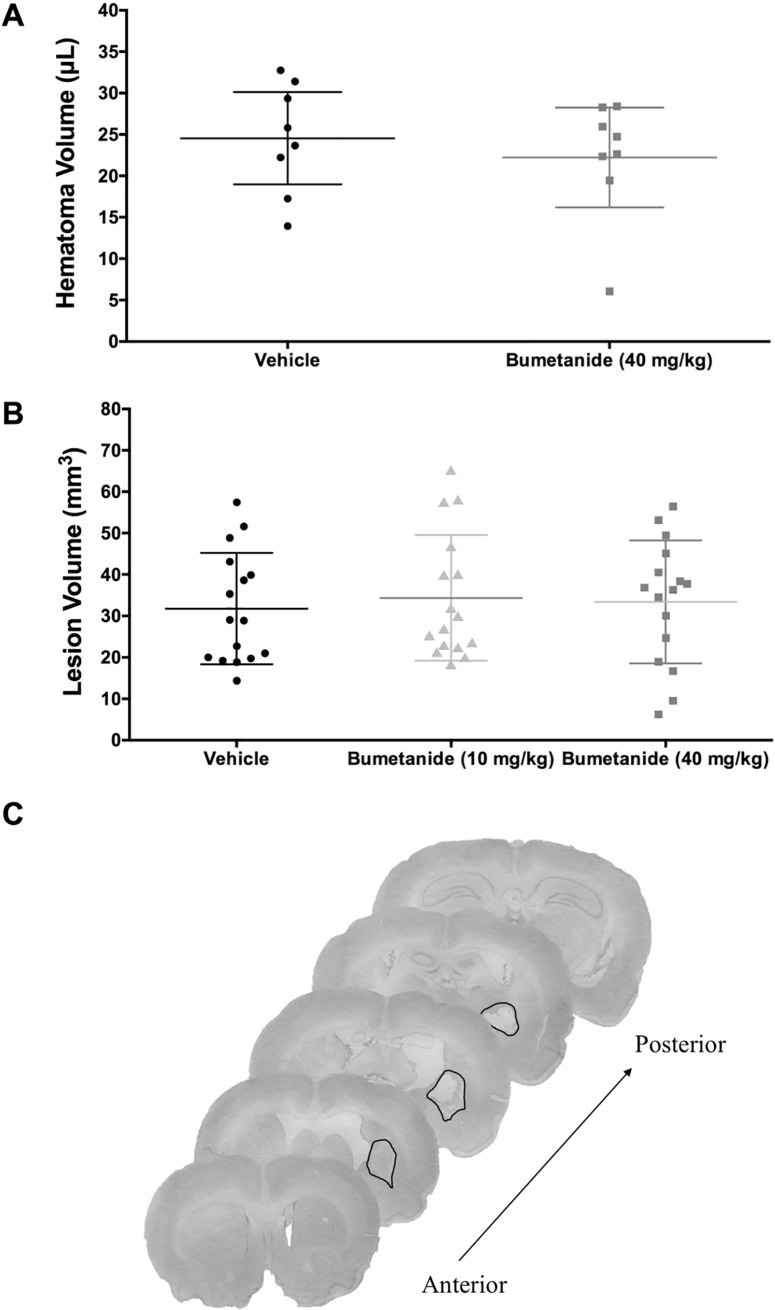
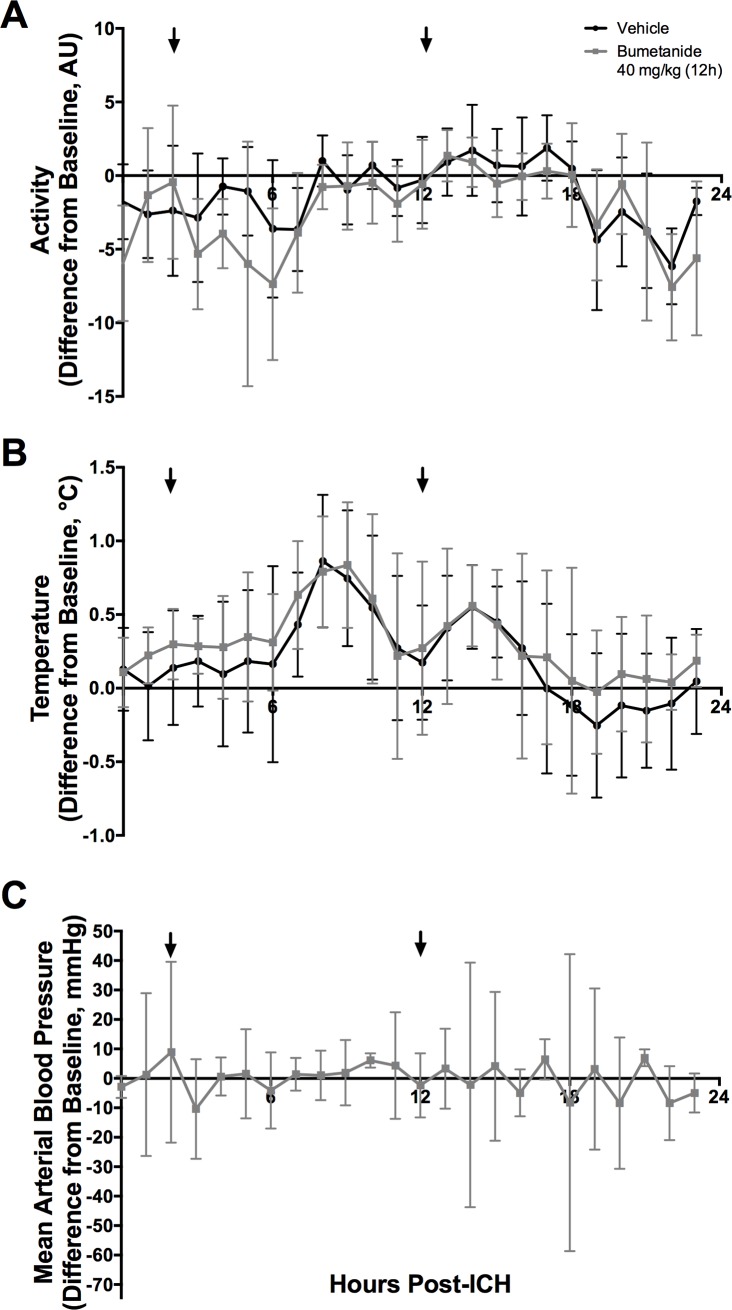
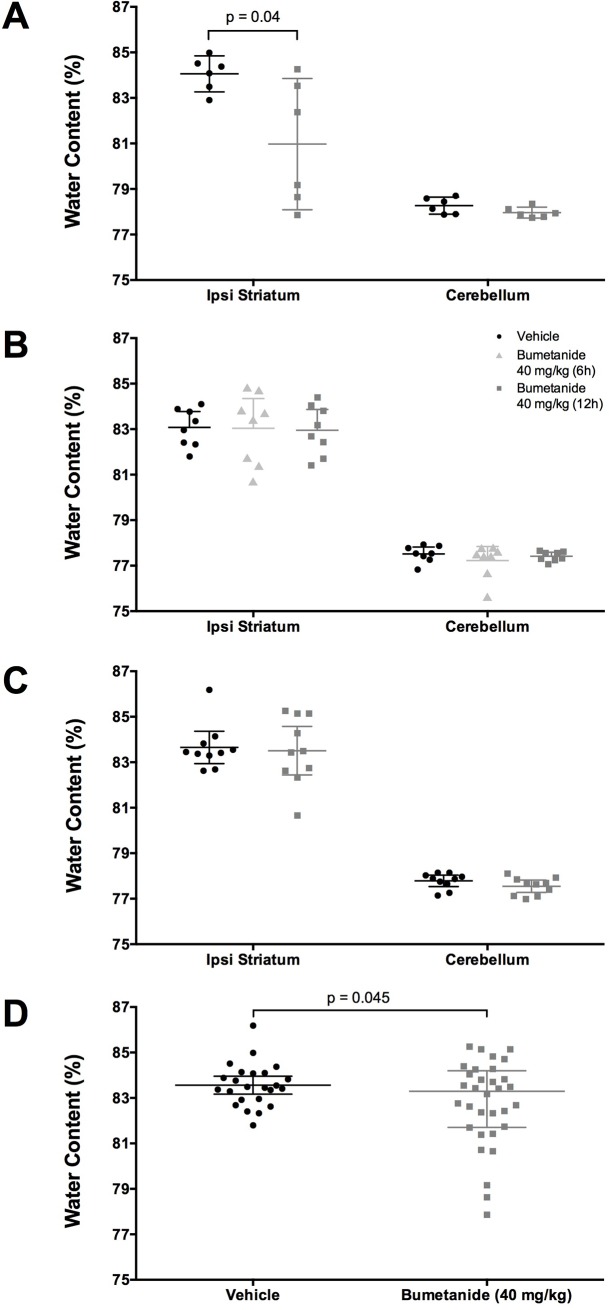
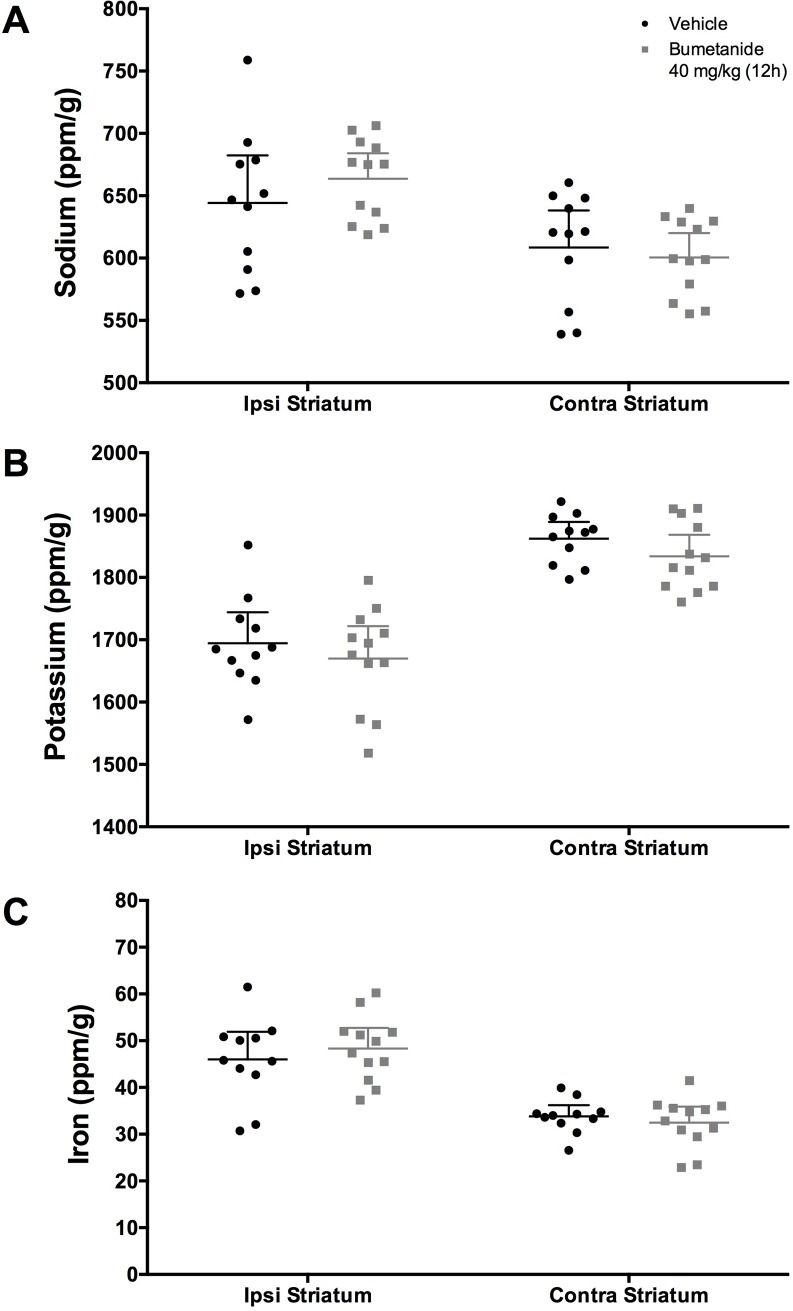
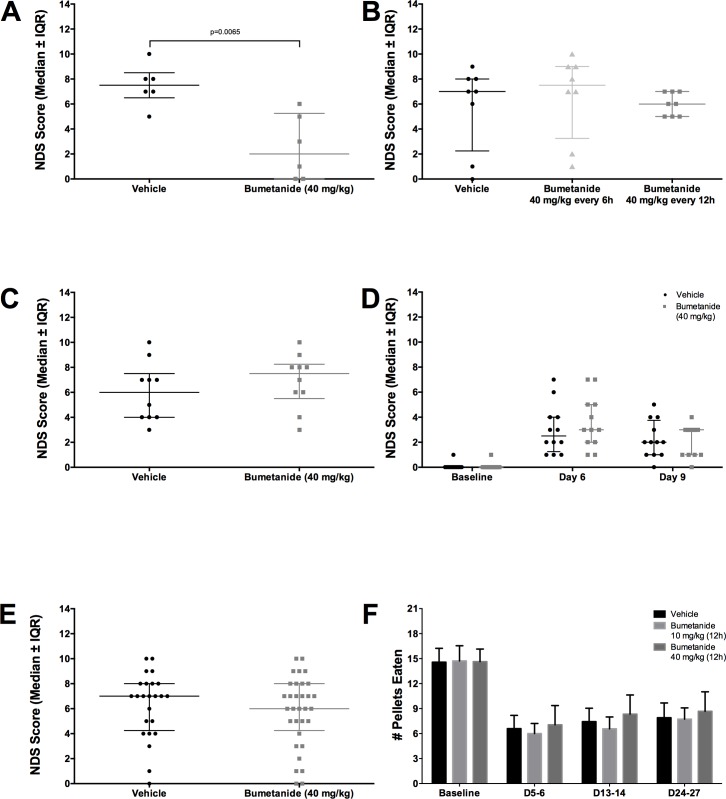
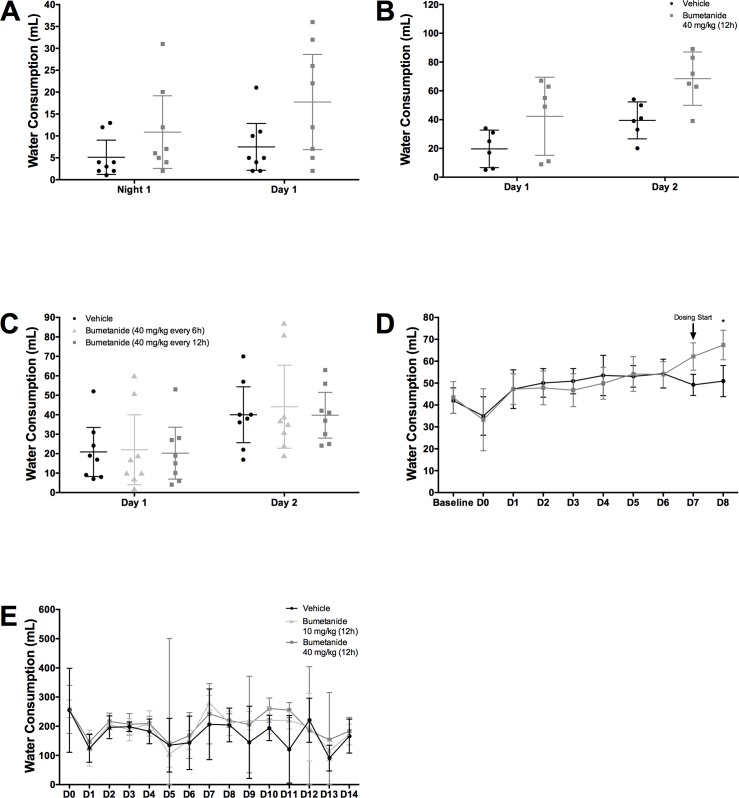
After intracerebral hemorrhage (ICH), brain edema commonly occurs and can cause death. Along with edema, there are significant alterations in the concentrations of key ions such as sodium, potassium, and chloride, which are essential to brain function. NKCC1, a cation-chloride cotransporter, is upregulated after brain damage, such as traumatic injury and ischemic stroke. NKCC1 brings sodium and chloride into the cell, possibly worsening ion dyshomeostasis. Bumetanide, a specific NKCC1 antagonist, blocks the transport of chloride into cells, and thus should attenuate the increases in chloride, which should lessen brain edema and improve neuronal functioning post-ICH, as with other injuries. We used the collagenase model of ICH to test whether bumetanide treatment for three days (vs. vehicle) would improve outcome. We gave bumetanide beginning at two hours or seven days post-ICH and measured behavioural outcome, edema, and brain ion content after treatment. There was some evidence for a minor reduction in edema after early dosing, but this did not improve behaviour or lessen injury. Contrary to our hypothesis, bumetanide did not normalize ion concentrations after late dosing. Bumetanide did not improve behavioural outcome or affect lesion volume. After ICH, bumetanide is safe to use in rats but does not improve functional outcome in the majority of animals.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Nadeau CA, Dietrich K, Wilkinson CM, Crawford AM, George GN, Nichol HK, et al. Prolonged Blood-Brain Barrier Injury Occurs After Experimental Intracerebral Hemorrhage and Is Not Acutely Associated with Additional Bleeding. Transl Stroke Res. Translational Stroke Research; 2018; 10.1007/s12975-018-0636-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
