

Lymph node positivity in different early breast carcinoma phenotypes: a predictive model
- PMID: 30630443
- PMCID: PMC6327612
- DOI: 10.1186/s12885-018-5227-3
Lymph node positivity in different early breast carcinoma phenotypes: a predictive model
Abstract
Background: A strong correlation between breast cancer (BC) molecular subtypes and axillary status has been shown. It would be useful to predict the probability of lymph node (LN) positivity.
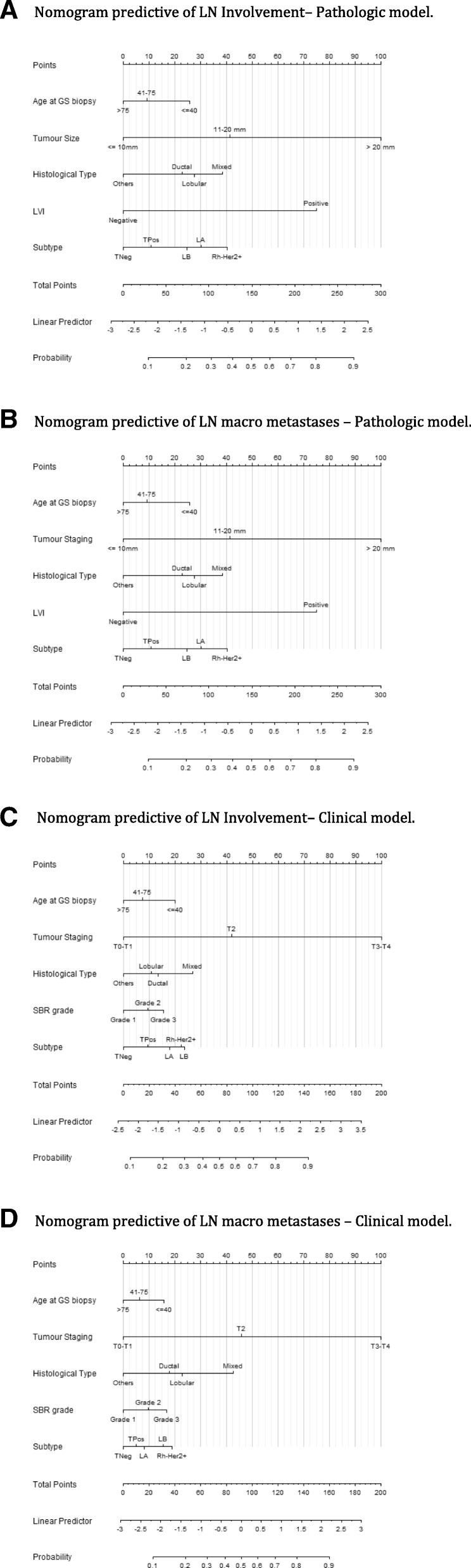
Objective: To develop the performance of multivariable models to predict LN metastases, including nomograms derived from logistic regression with clinical, pathologic variables provided by tumor surgical results or only by biopsy.
Methods: A retrospective cohort was randomly divided into two separate patient sets: a training set and a validation set. In the training set, we used multivariable logistic regression techniques to build different predictive nomograms for the risk of developing LN metastases. The discrimination ability and calibration accuracy of the resulting nomograms were evaluated on the training and validation set.
Results: Consecutive sample of 12,572 early BC patients with sentinel node biopsies and no neoadjuvant therapy. In our predictive macro metastases LN model, the areas under curve (AUC) values were 0.780 and 0.717 respectively for pathologic and pre-operative model, with a good calibration, and results with validation data set were similar: AUC respectively of 0.796 and 0.725. Among the list of candidate's regression variables, on the training set we identified age, tumor size, LVI, and molecular subtype as statistically significant factors for predicting the risk of LN metastases.
Conclusions: Several nomograms were reported to predict risk of SLN involvement and NSN involvement. We propose a new calculation model to assess this risk of positive LN with similar performance which could be useful to choose management strategies, to avoid axillary LN staging or to propose ALND for patients with high level probability of major axillary LN involvement but also to propose immediate breast reconstruction when post mastectomy radiotherapy is not required for patients without LN macro metastasis.
Keywords: Breast cancer; Molecular subtype; Nomogram; Risk prediction; Sentinel node.
Conflict of interest statement
Ethics approval and consent to participate
This work was approved by our institutional review board (
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, Costantino JP, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010;11:927–933. doi: 10.1016/S1470-2045(10)70207-2. - DOI - PMC - PubMed
-
- Galimberti V, Cole BF, Zurrida S, Viale G, Luini A, Veronesi P, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. Lancet Oncol. 2013;14:297–305. doi: 10.1016/S1470-2045(13)70035-4. - DOI - PMC - PubMed
-
- Friedman D, Gipponi M, Murelli F, Meszaros P, Solari N, Massa M, et al. Predictive factors of non-sentinel lymph node involvement in patients with invasive breast cancer and sentinel node micrometastases. Anticancer Res. 2013;33:4509–4514. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
