

Morbidity, mortality and missed appointments in healthcare: a national retrospective data linkage study
- PMID: 30630493
- PMCID: PMC6329132
- DOI: 10.1186/s12916-018-1234-0
Morbidity, mortality and missed appointments in healthcare: a national retrospective data linkage study
Abstract
Background: Recently, studies have examined the underlying patient and practice factors for missed appointments, but less is known about the impact on patient health. People with one or more long-term conditions who fail to attend appointments may be at risk of premature death. This is the first study to examine the effect of missed primary healthcare appointments on all-cause mortality in those with long-term mental and physical health conditions.
Methods: We used a large, nationwide retrospective cohort (n = 824,374) extracted from routinely collected general practice data across Scotland over a 3-year period from September 2013 until September 2016. This data encompasses appointment history for approximately 15% of the Scottish population, and was linked to Scottish deaths records for patients who had died within a 16-month follow-up period. We generated appointment attendance history, number of long-term conditions and prescriptions data for patients. These factors were used in negative binomial and Cox's proportional hazards modelling to examine the risk of missing appointments and all-cause mortality.
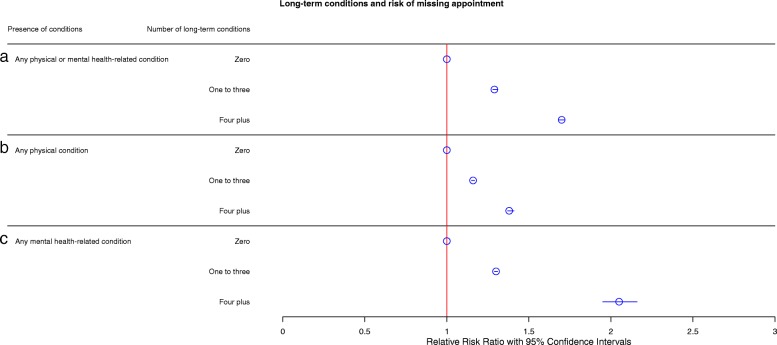
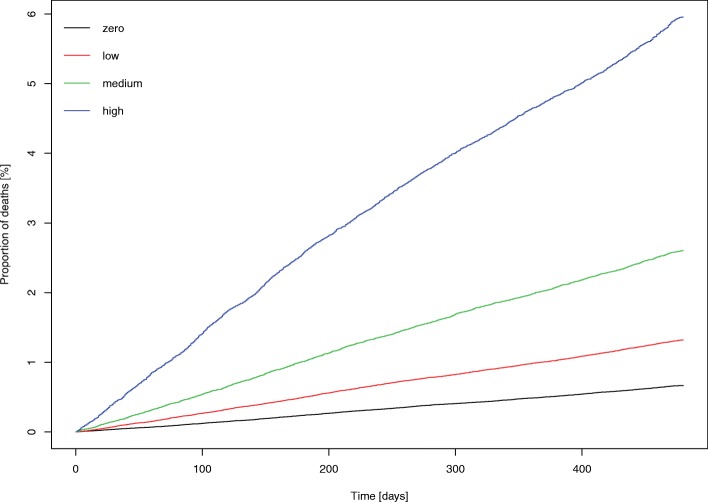
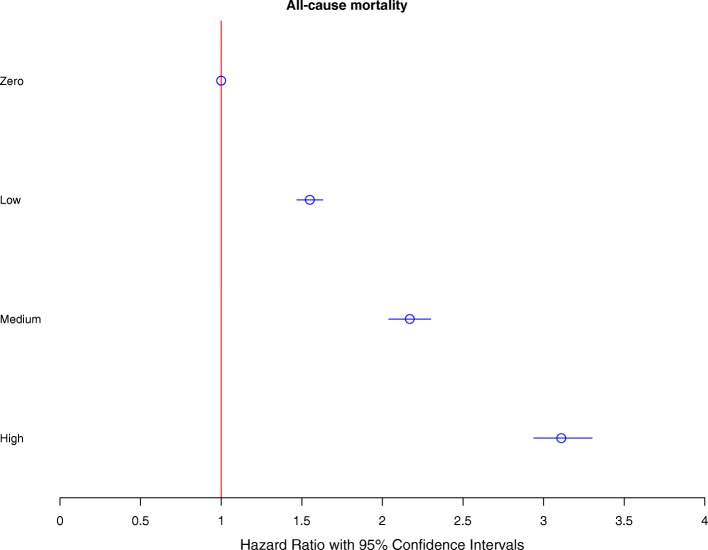
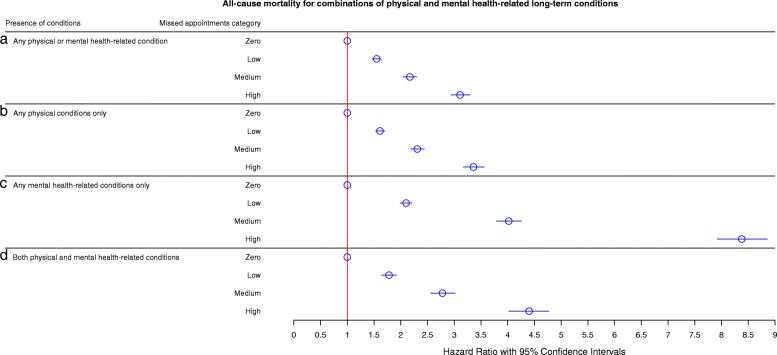
Results: Patients with a greater number of long-term conditions had an increased risk of missing general practice appointments despite controlling for number of appointments made, particularly among patients with mental health conditions. These patients were at significantly greater risk of all-cause mortality, and showed a dose-based response with increasing number of missed appointments. Patients with long-term mental health conditions who missed more than two appointments per year had a greater than 8-fold increase in risk of all-cause mortality compared with those who missed no appointments. These patients died prematurely, commonly from non-natural external factors such as suicide.
Conclusions: Missed appointments represent a significant risk marker for all-cause mortality, particularly in patients with mental health conditions. For these patients, existing primary healthcare appointment systems are ineffective. Future interventions should be developed with a particular focus on increasing attendance by these patients.
Keywords: Missed appointments; administrative data; health inequalities; health promotion; health utilisation; long-term conditions; morbidity; mortality; primary care; social vulnerability.
Conflict of interest statement
Ethical approval
Letters of comfort were issued by the West of Scotland NHS Ethics Committee and the University of Glasgow College of Medical, Veterinary & Life Sciences Ethics Committee confirming that the full study did not need NHS ethics permission. Public Benefit and Privacy Panel approval was granted by NHS Information Services Scotland in December 2016. Data were aggregated where necessary to ensure individual patient privacy.
Consent for publication
No personal information was given so consent to publish was not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Missed GP appointments linked to higher risk of death.BMJ. 2019 Feb 5;364:l485. doi: 10.1136/bmj.l485. BMJ. 2019. PMID: 30723085 No abstract available.
References
-
- Salisbury C, Mercer S, Fortin M. The ABC of Multimorbidity. Oxford: Wiley-Blackwell; 2014.
-
- van Oostrom SH, Gijsen R, Stirbu I, Korevaar JC, Schellevis FG, Picavet HSJ, et al. Time trends in prevalence of chronic diseases and multimorbidity not only due to aging: data from general practices and health surveys. PLoS One. 2016;11(8):e0160264. doi: 10.1371/journal.pone.0160264. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
