

Duration of asymptomatic status and outcomes following carotid endarterectomy and carotid artery stenting in the Carotid Revascularization Endarterectomy vs Stenting Trial
- PMID: 30630649
- PMCID: PMC6548589
- DOI: 10.1016/j.jvs.2018.09.054
Duration of asymptomatic status and outcomes following carotid endarterectomy and carotid artery stenting in the Carotid Revascularization Endarterectomy vs Stenting Trial
Abstract
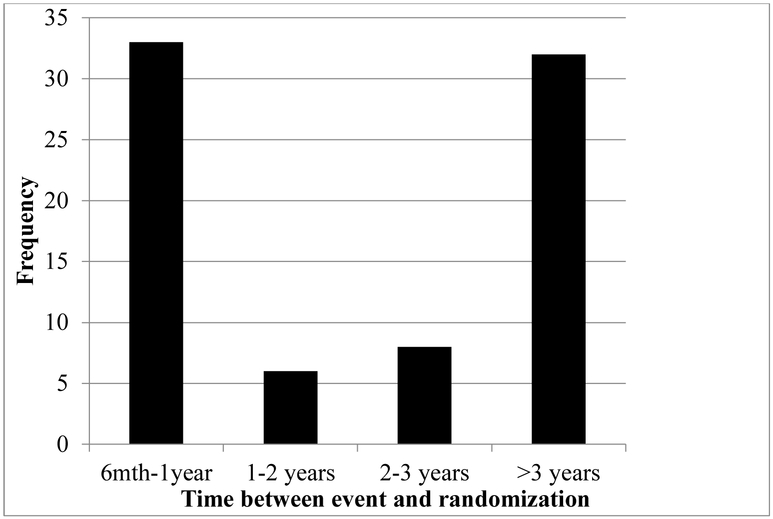
Background: Most carotid revascularization studies define asymptomatic as symptom-free for more than 180 days; however, it is unknown if intervention carries similar risk among those currently asymptomatic but with previous symptoms (PS) vs those who were always asymptomatic (AA).
Methods: We compared the periprocedural and 4-year risks of PS vs AA patients in the Carotid Revascularization Endarterectomy vs Stenting Trial (CREST) randomized to carotid endarterectomy (CEA) or carotid artery stenting (CAS)/angioplasty. Proportional hazards models adjusting for age, sex, and treatment were used to assess the risk of periprocedural stroke and/or death (S+D; any S+D during periprocedural period), stroke and death at 4 years (any S+D within the periprocedural period and ipsilateral stroke out to 4 years) and the primary end point at 4 years (any stroke, death, and myocardial infarction within the periprocedural period and ipsilateral stroke out to 4 years). Analysis was performed pooling the CEA-treated and CAS-treated patients, and separately for each treatment.
Results: Of 1181 asymptomatic patients randomized in CREST, 1104 (93%) were AA and 77 (7%) were PS. There was no difference in risk when comparing the AA and PS cohorts in the pooled CAS+CEA population for periprocedural S+D (2.0% vs 1.3%), S+D at 4 years (3.6% vs 3.2%), or the primary end point (5.2% vs 5.8%). There were also no differences among those assigned to CEA (periprocedural S+D, 1.5% vs 0%; S+D at 4 years, 2.7% vs 0%; or primary end point, 5.1% vs 2.4%) or CAS (periprocedural S+D, 2.5% vs 2.8%; S+D at 4 years, 4.4% vs 6.9%; or primary end point, 5.3% vs 9.8%) when analyzed separately.
Conclusions: In CREST, only a small minority of asymptomatic patients had previous ipsilateral symptoms. The outcomes of periprocedural S+D, periprocedural S+D, and ipsilateral stroke up to 4 years, and the primary end point did not differ for AA patients compared with PS patients.
Trial registration: ClinicalTrials.gov NCT00004732.
Keywords: Asymptomatic patients; Carotid stenosis; Prior symptoms in asymptomatic patients.
Copyright © 2018 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURE
G. Roubin - Royalties: Cook Inc.; Ownership interest: Essential Medical.
All other authors - None.
Figures
References
-
- Bond R, Rerkasem K, Naylor AR, Aburahma AF, Rothwell PM. Systematic review of randomized controlled trials of patch angioplasty versus primary closure and different types of patch materials during carotid endarterectomy. J Vasc Surg. 2004;40:1126–1135 - PubMed
-
- Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL, et al. 2011 asa/accf/aha/aann/aans/acr/asnr/cns/saip/scai/sir/snis/svm/svs guideline on the management of patients with extracranial carotid and vertebral artery disease: Executive summary: A report of the american college of cardiology foundation/american heart association task force on practice guidelines, and the american stroke association, american association of neuroscience nurses, american association of neurological surgeons, american college of radiology, american society of neuroradiology, congress of neurological surgeons, society of atherosclerosis imaging and prevention, society for cardiovascular angiography and interventions, society of interventional radiology, society of neurointerventional surgery, society for vascular medicine, and society for vascular surgery. Developed in collaboration with the american academy of neurology and society of cardiovascular computed tomography. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2013;81:E76–123 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
