

Adiposity and risk of decline in glomerular filtration rate: meta-analysis of individual participant data in a global consortium
- PMID: 30630856
- PMCID: PMC6481269
- DOI: 10.1136/bmj.k5301
Adiposity and risk of decline in glomerular filtration rate: meta-analysis of individual participant data in a global consortium
Abstract
Objective: To evaluate the associations between adiposity measures (body mass index, waist circumference, and waist-to-height ratio) with decline in glomerular filtration rate (GFR) and with all cause mortality.
Design: Individual participant data meta-analysis.
Setting: Cohorts from 40 countries with data collected between 1970 and 2017.
Participants: Adults in 39 general population cohorts (n=5 459 014), of which 21 (n=594 496) had data on waist circumference; six cohorts with high cardiovascular risk (n=84 417); and 18 cohorts with chronic kidney disease (n=91 607).
Main outcome measures: GFR decline (estimated GFR decline ≥40%, initiation of kidney replacement therapy or estimated GFR <10 mL/min/1.73 m2) and all cause mortality.
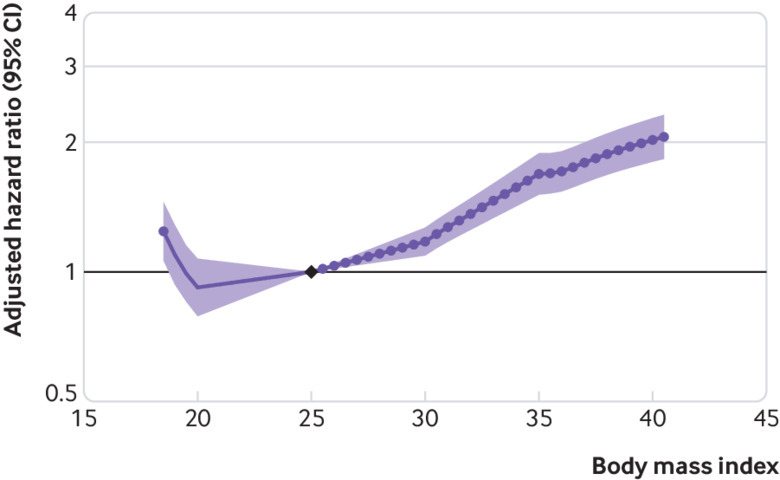
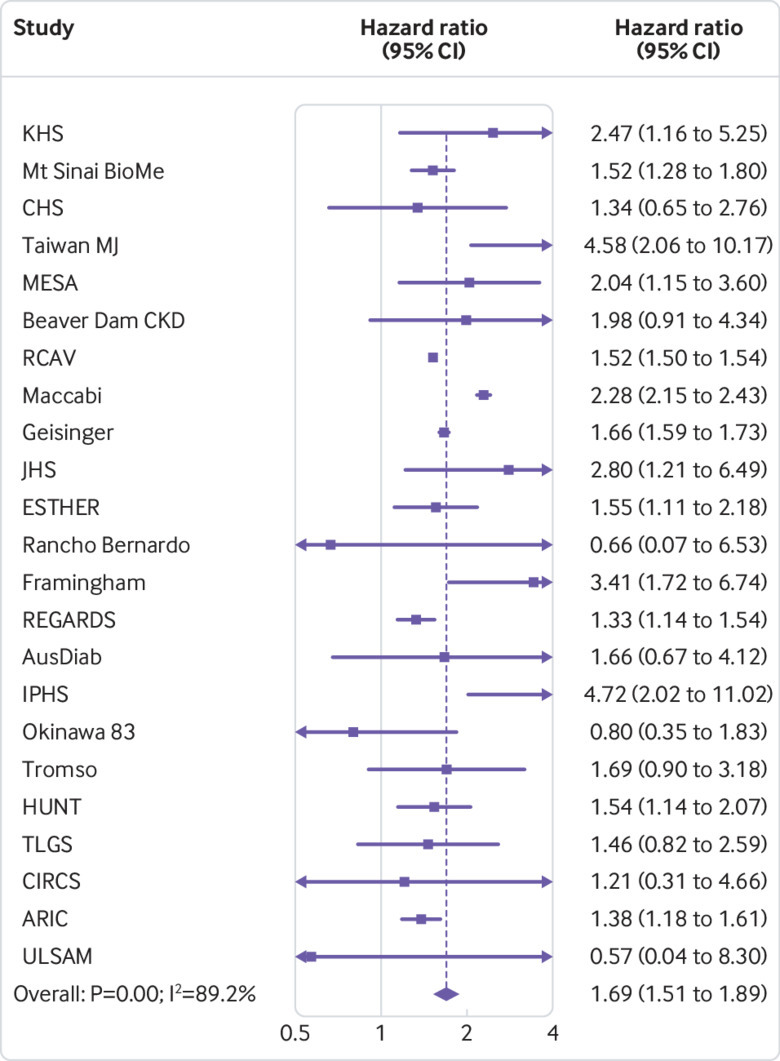
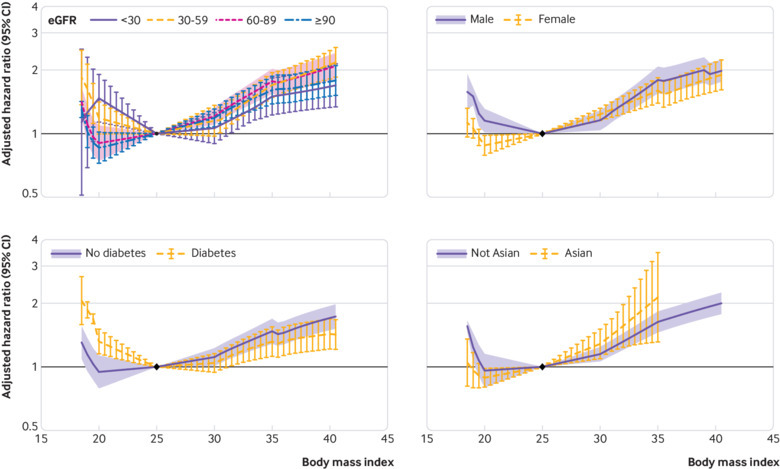
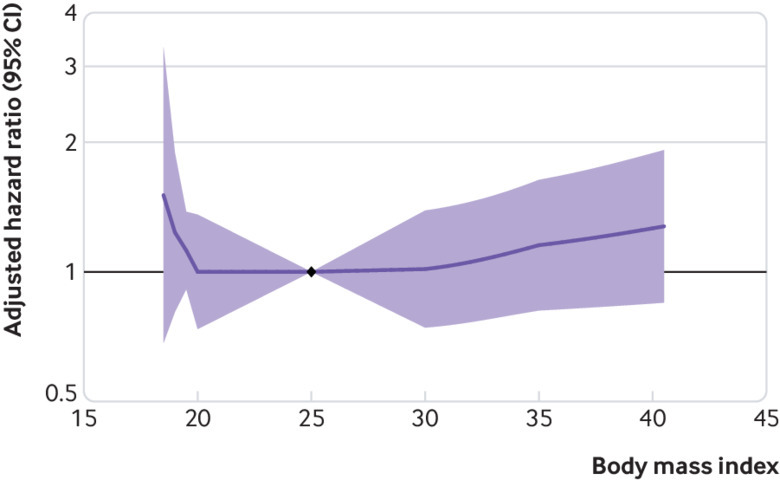
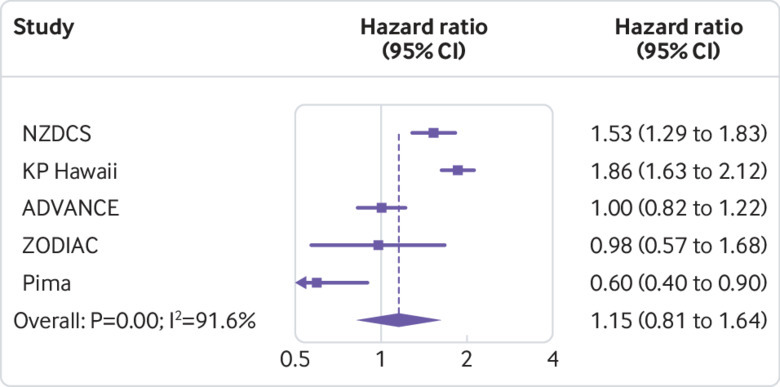
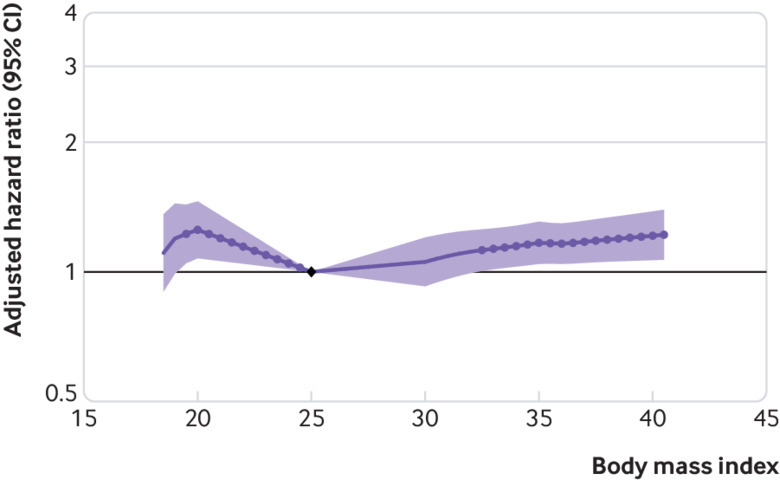
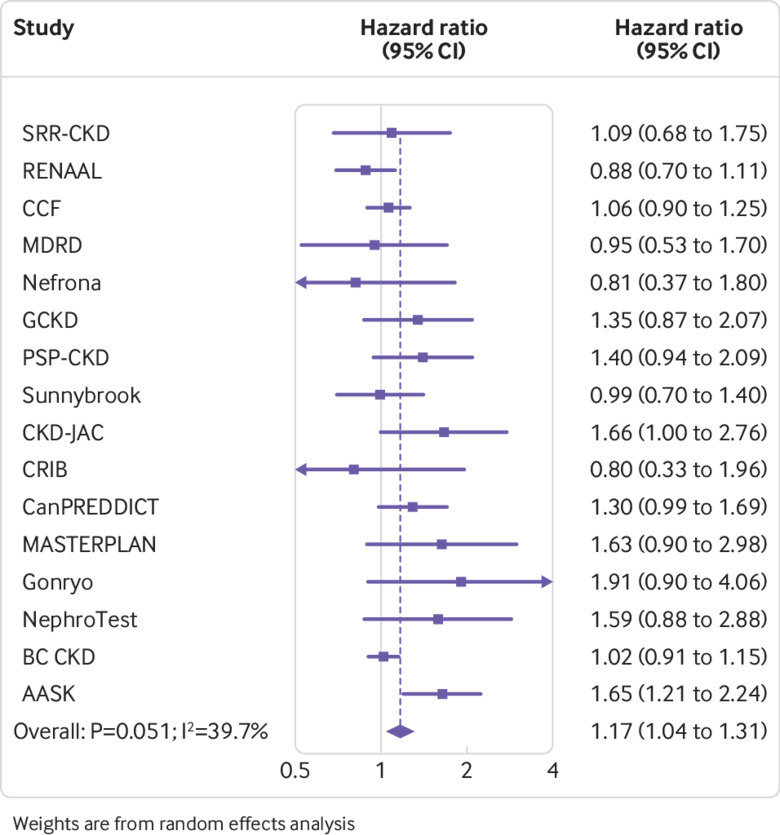
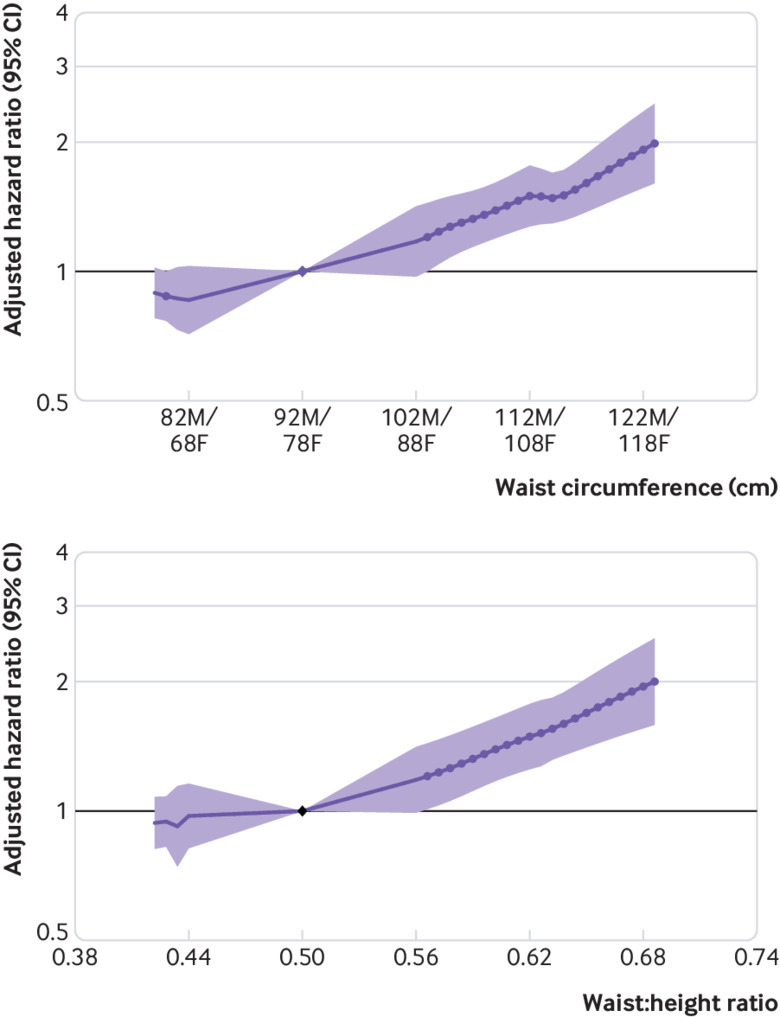
Results: Over a mean follow-up of eight years, 246 607 (5.6%) individuals in the general population cohorts had GFR decline (18 118 (0.4%) end stage kidney disease events) and 782 329 (14.7%) died. Adjusting for age, sex, race, and current smoking, the hazard ratios for GFR decline comparing body mass indices 30, 35, and 40 with body mass index 25 were 1.18 (95% confidence interval 1.09 to 1.27), 1.69 (1.51 to 1.89), and 2.02 (1.80 to 2.27), respectively. Results were similar in all subgroups of estimated GFR. Associations weakened after adjustment for additional comorbidities, with respective hazard ratios of 1.03 (0.95 to 1.11), 1.28 (1.14 to 1.44), and 1.46 (1.28 to 1.67). The association between body mass index and death was J shaped, with the lowest risk at body mass index of 25. In the cohorts with high cardiovascular risk and chronic kidney disease (mean follow-up of six and four years, respectively), risk associations between higher body mass index and GFR decline were weaker than in the general population, and the association between body mass index and death was also J shaped, with the lowest risk between body mass index 25 and 30. In all cohort types, associations between higher waist circumference and higher waist-to-height ratio with GFR decline were similar to that of body mass index; however, increased risk of death was not associated with lower waist circumference or waist-to-height ratio, as was seen with body mass index.
Conclusions: Elevated body mass index, waist circumference, and waist-to-height ratio are independent risk factors for GFR decline and death in individuals who have normal or reduced levels of estimated GFR.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: part support from the US National Kidney Foundation and the National Institute of Diabetes and Digestive and Kidney Diseases for the submitted work; ARC was supported by the NIDDK; no other financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activites that could appear to have influenced the submitted work.
Figures
References
-
- United States Renal Data System 2017 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2017.
-
- Hsu CY, McCulloch CE, Iribarren C, Darbinian J, Go AS. Body mass index and risk for end-stage renal disease. Ann Intern Med 2006;144:21-8. - PubMed