

Automatic Coronary Wall and Atherosclerotic Plaque Segmentation from 3D Coronary CT Angiography
- PMID: 30631101
- PMCID: PMC6328572
- DOI: 10.1038/s41598-018-37168-4
Automatic Coronary Wall and Atherosclerotic Plaque Segmentation from 3D Coronary CT Angiography
Abstract
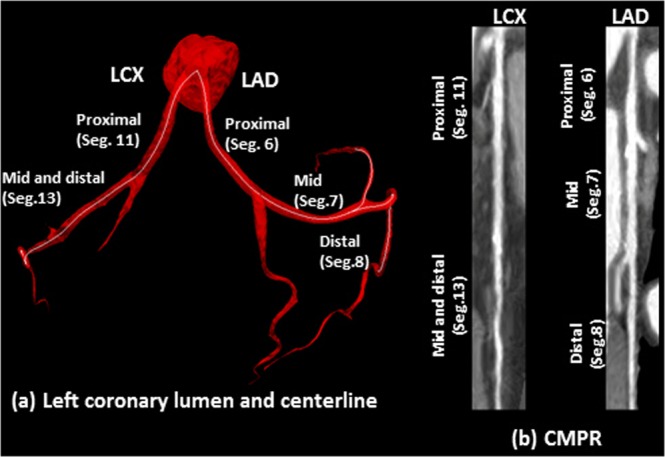
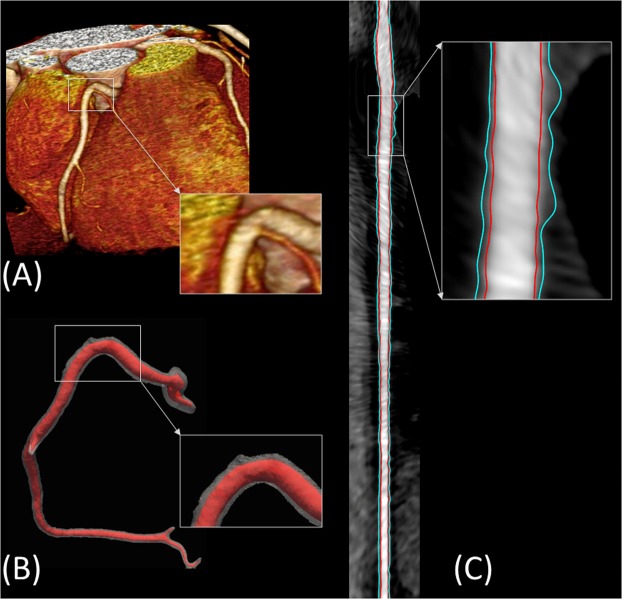
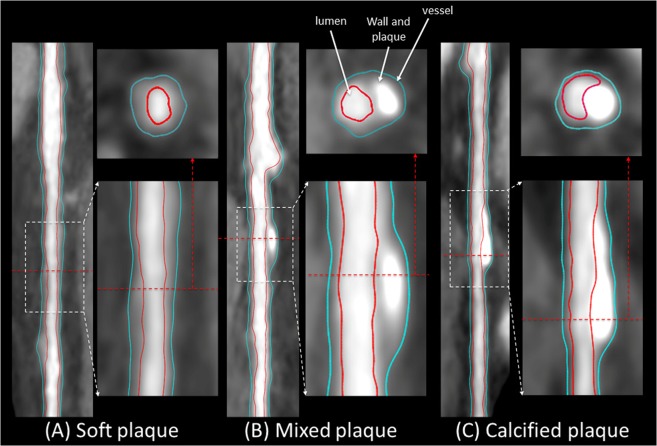
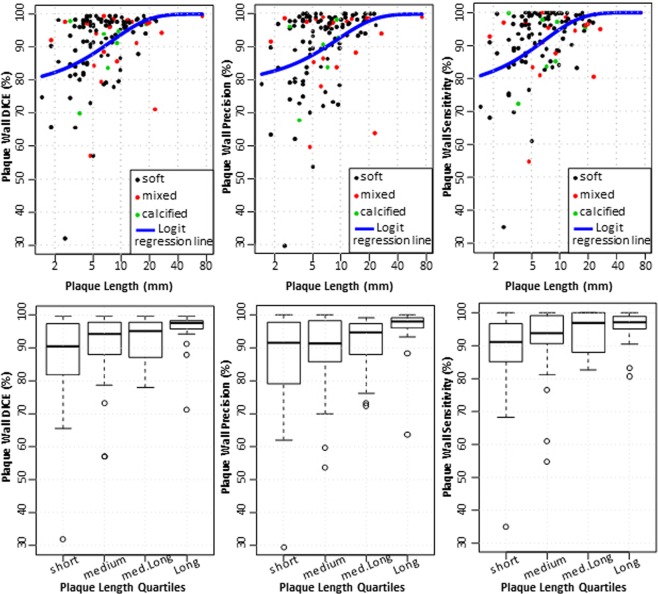
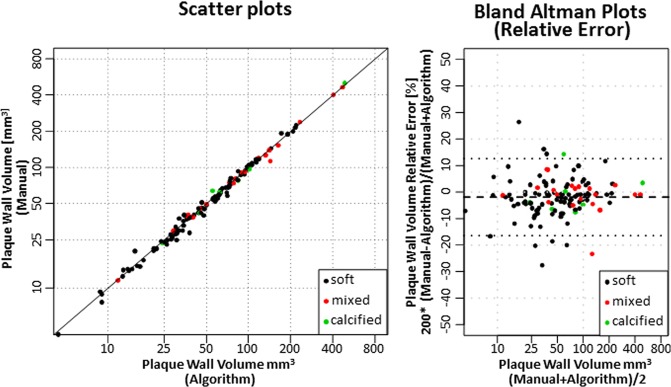
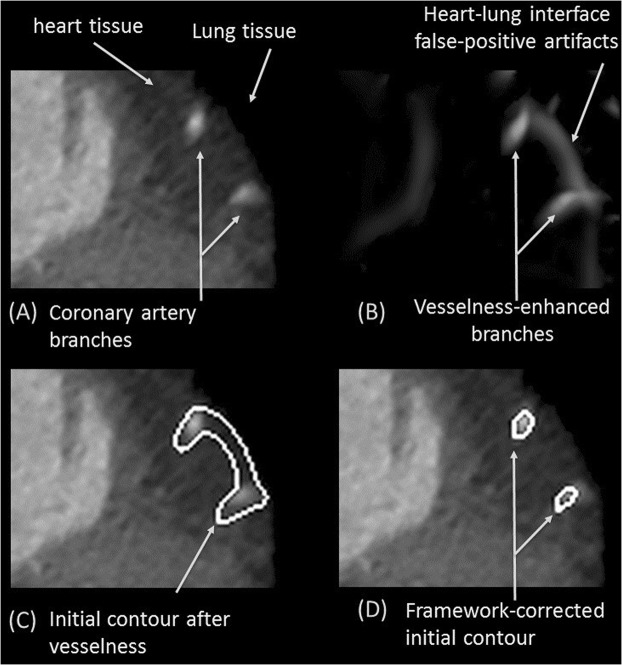
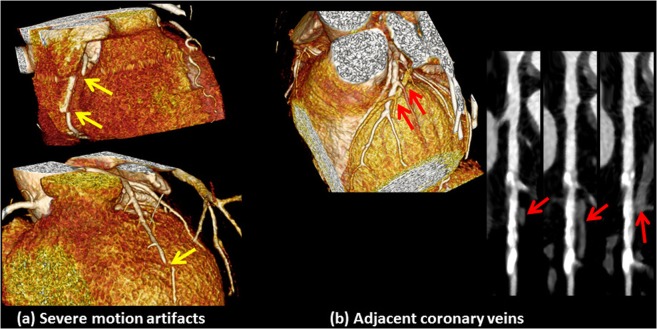
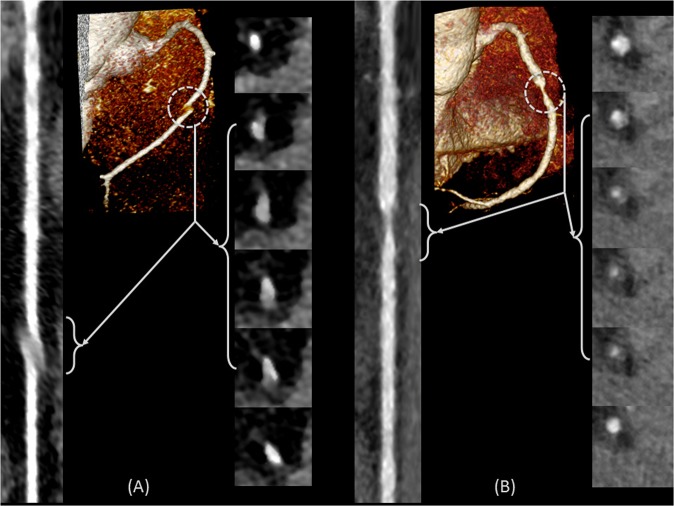
Coronary plaque burden measured by coronary computerized tomography angiography (CCTA), independent of stenosis, is a significant independent predictor of coronary heart disease (CHD) events and mortality. Hence, it is essential to develop comprehensive CCTA plaque quantification beyond existing subjective plaque volume or stenosis scoring methods. The purpose of this study is to develop a framework for automated 3D segmentation of CCTA vessel wall and quantification of atherosclerotic plaque, independent of the amount of stenosis, along with overcoming challenges caused by poor contrast, motion artifacts, severe stenosis, and degradation of image quality. Vesselness, region growing, and two sequential level sets are employed for segmenting the inner and outer wall to prevent artifact-defective segmentation. Lumen and vessel boundaries are joined to create the coronary wall. Curved multiplanar reformation is used to straighten the segmented lumen and wall using lumen centerline. In-vivo evaluation included CCTA stenotic and non-stenotic plaques from 41 asymptomatic subjects with 122 plaques of different characteristics against the individual and consensus of expert readers. Results demonstrate that the framework segmentation performed robustly by providing a reliable working platform for accelerated, objective, and reproducible atherosclerotic plaque characterization beyond subjective assessment of stenosis; can be potentially applicable for monitoring response to therapy.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Mortality GBD. & Causes of Death, C. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. doi: 10.1016/S0140-6736(14)61682-2. - DOI - PMC - PubMed
-
- Sangiorgi G, et al. Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: a histologic study of 723 coronary artery segments using nondecalcifying methodology. Journal of the American College of Cardiology. 1998;31:126–133. doi: 10.1016/S0735-1097(97)00443-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
