

Mills' syndrome revisited
- PMID: 30631918
- PMCID: PMC6394692
- DOI: 10.1007/s00415-019-09186-3
Mills' syndrome revisited
Abstract
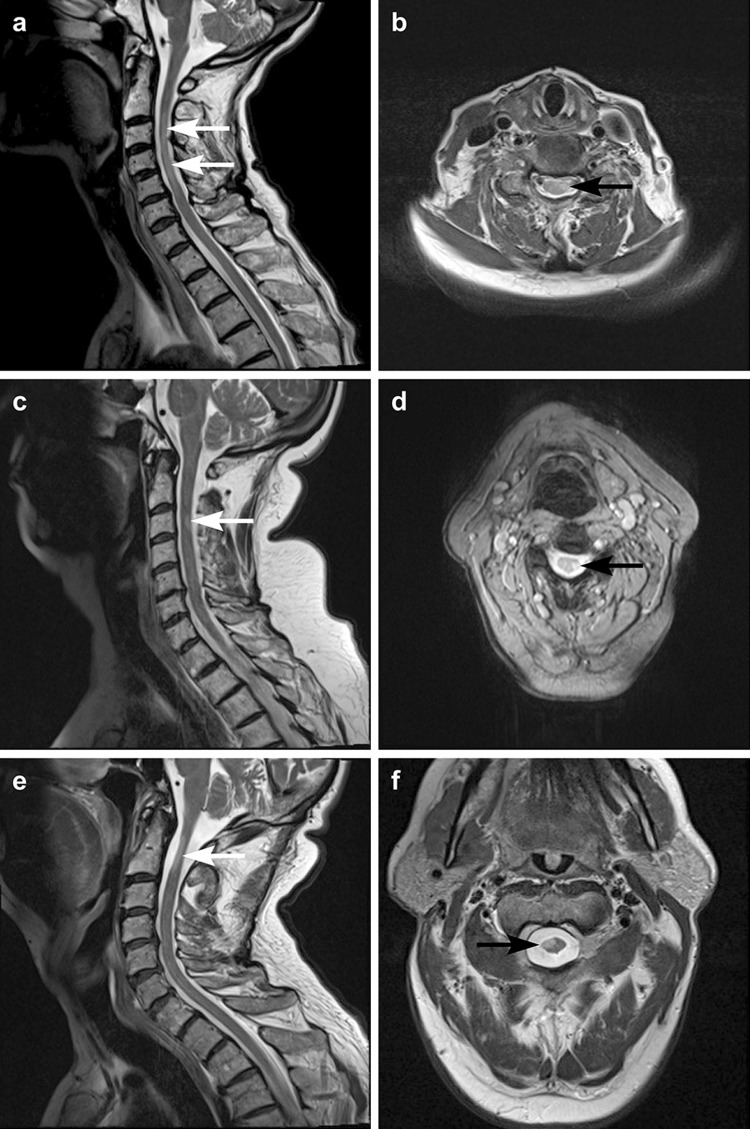
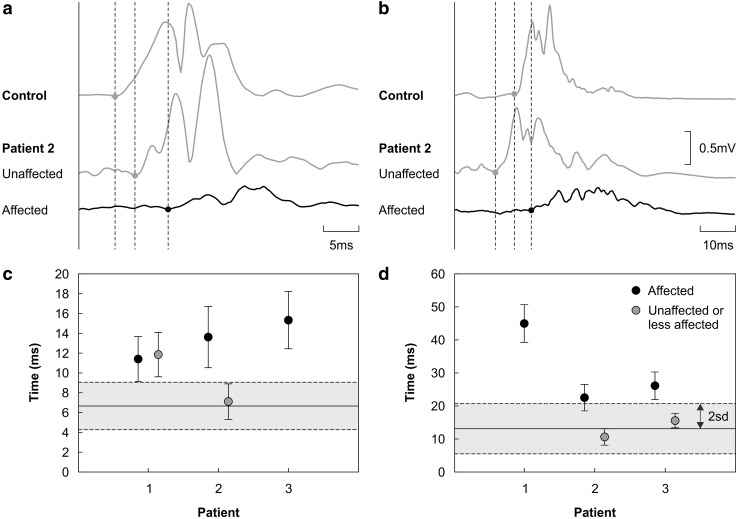
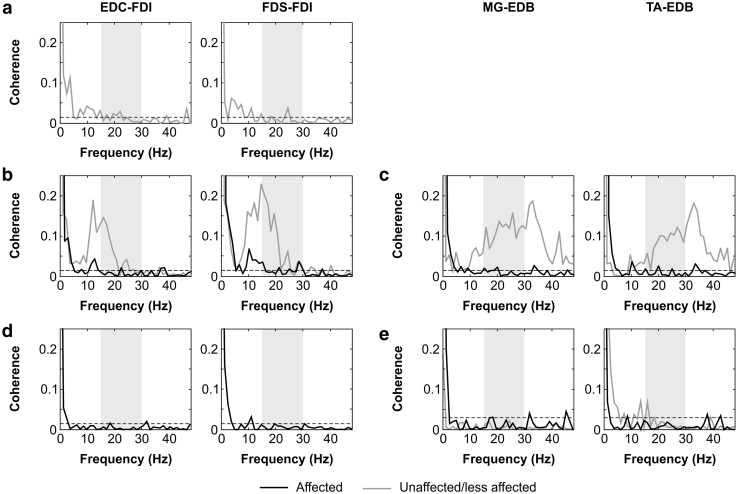
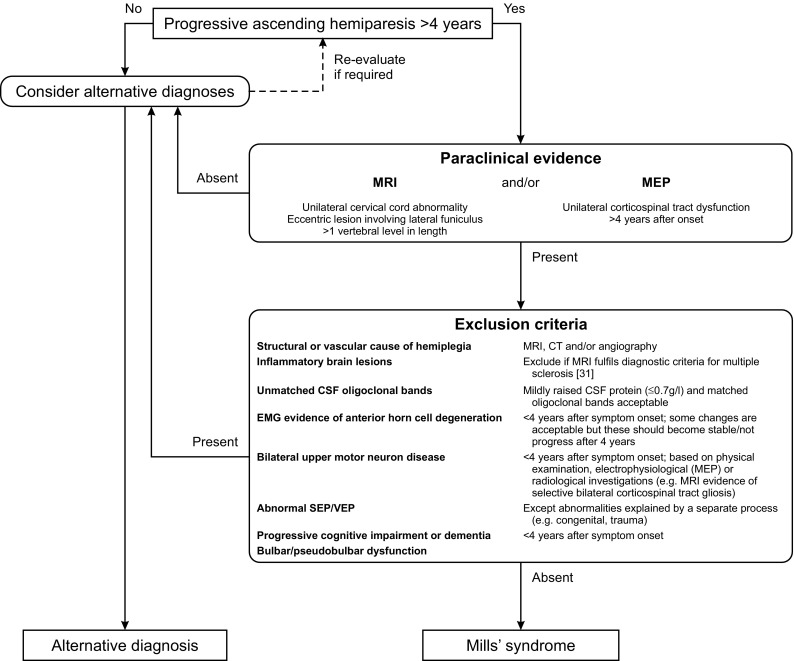
Mills' syndrome is an idiopathic, slowly progressive, spastic hemiparesis. We describe three cases that have been under review for a minimum of 11 years (range 11-19). In all patients, symptoms started in a leg, with a mean age of onset of 59 years (range 53-63). The only abnormality on laboratory investigations was a mildly elevated CSF protein in one case. MRI demonstrated focal T2 hyper-intensity located eccentrically in the cervical cord ipsilateral to the symptomatic side. No cerebral abnormality was demonstrated. Whilst visual and somatosensory evoked potentials were unremarkable, motor evoked potentials were abnormal in all patients: central motor conduction times were significantly prolonged unilaterally in two patients and bilaterally but asymmetrically in the third. Beta-band (15-30 Hz) intermuscular coherence, a potentially more sensitive method of assessing upper motor neuron integrity, was absent unilaterally in one patient and bilaterally in the other two. One patient developed amyotrophy and thus a picture of amyotrophic lateral sclerosis after 16 years, suggesting that Mills' syndrome is part of the motor neuron disease spectrum. Both amyotrophy and subclinical contralateral upper motor neuron disease can therefore be features of Mills' syndrome. However, even with the most sensitive electrodiagnostic techniques, unilateral upper motor neuron disease can remain the only abnormality for as long as 10 years. We conclude that whilst Mills' syndrome should be classified as a motor neuron disorder, it is a distinct nosological entity which can be distinguished from amyotrophic lateral sclerosis, upper motor neuron-dominant amyotrophic lateral sclerosis and primary lateral sclerosis. We propose diagnostic criteria for Mills' syndrome, and estimate a point prevalence of at least 1.2:1,000,000 based on our well-defined referral population in the North of England.
Keywords: MRI; Mills’ syndrome; Neurophysiology; Spastic hemiparesis.
Conflict of interest statement
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standards
Most investigations were carried out as part of routine clinical care. Studies of motor cortical evoked potentials (MEP) and coherence were approved by the local NHS research ethics committee (approval number 08/H0908/3) and conformed to the Declaration of Helsinki.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
