

Using health-related quality of life to predict cardiovascular disease events
- PMID: 30632050
- PMCID: PMC7830778
- DOI: 10.1007/s11136-019-02103-1
Using health-related quality of life to predict cardiovascular disease events
Abstract
Purpose: Although strong associations between self-reported health and mortality exist, quality of life is not conceptualized as a cardiovascular disease (CVD) risk factor. Our objective was to assess the independent association between health-related quality of life (HRQOL) and incident CVD.
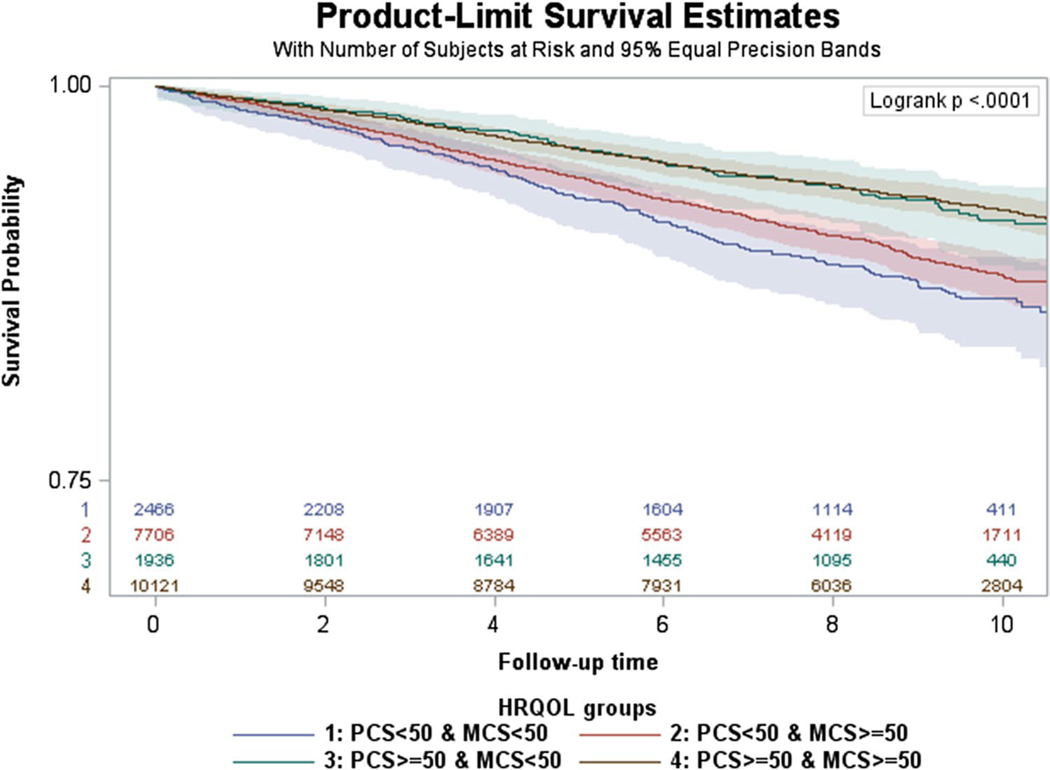
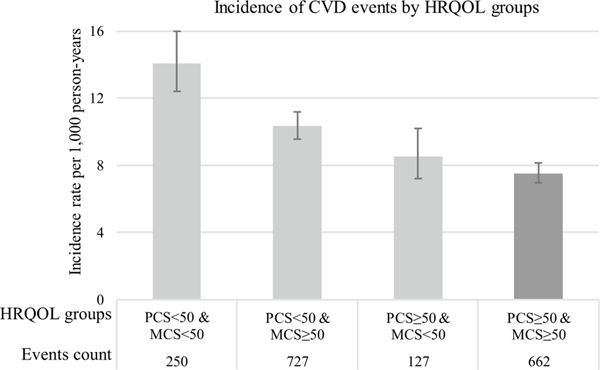
Methods: This study used the REasons for Geographic And Racial Differences in Stroke data, which enrolled 30,239 adults from 2003 to 2007 and followed them over 10 years. We included 22,229 adults with no CVD history at baseline. HRQOL was measured using the SF-12 Physical Component Summary (PCS) and Mental Component Summary (MCS) scores, which range from 0 to 100, with higher scores indicating better HRQOL. Scores were normed to the general US population with mean 50 and standard deviation 10. We constructed a four-level HRQOL variable: (1) individuals with PCS & MCS < 50, (2) PCS < 50 & MCS ≥ 50, (3) MCS < 50 & PCS ≥ 50, and (4) PCS & MCS ≥ 50, which was the reference. The primary outcome was incident CVD (non-fatal myocardial infarction (MI), fatal MI or coronary heart disease (CHD) death, fatal and non-fatal stroke). Cox proportional hazards models examined associations between HRQOL and CVD.
Results: Median follow-up was 8.4 (IQR 5.9-10.0) years. We observed 1766 CVD events. Compared to having PCS & MCS ≥ 50, having MCS & PCS < 50 was associated with increased CVD risk (aHR 1.46; 95% 1.24-1.70), adjusting for demographics, comorbidities, and CVD risk factors. Associations between MCS & PCS < 50 and CVD were consistent for CHD (aHR 1.54 [1.26-1.89]) and stroke (aHR 1.35 [1.05-1.72]) endpoints.
Conclusions: Given strong, adjusted associations between poor HRQOL and incident CVD, self-reported health may be an excellent complement to current approaches to CVD risk identification.
Keywords: Cardiovascular events; Quality of life; Risk assessments.
Conflict of interest statement
Figures
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, & Muntner P. (2017). Heart disease and stroke statistics-2017 update: A report From the American Heart Association. Circulation, 135(10), e146–e603. 10.1161/cir.0000000000000485. - DOI - PMC - PubMed
-
- Goff DC Jr., Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB Sr., Gibbons R, Greenland P, Lackland DT, Levy D, O’Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC Jr., Sorlie P, Stone NJ, & Wilson PW (2014). 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology, 63(25 Pt B), 2935–2959. 10.1016/j.jacc.2013.11.005. - DOI - PMC - PubMed
-
- Colantonio LD, Richman JS, Carson AP, Lloyd-Jones DM, Howard G, Deng L, Howard VJ, Safford MM, Muntner P, & Goff DC Jr. (2017) Performance of the atherosclerotic cardiovascular disease pooled cohort risk equations by social deprivation status. Journal of the American Heart Association. 10.1161/jaha.117.005676. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
