

Prognostic value of pretreatment lymphocyte-to-monocyte ratio in patients with urologic tumors: A PRISMA-compliant meta-analysis
- PMID: 30633220
- PMCID: PMC6336582
- DOI: 10.1097/MD.0000000000014091
Prognostic value of pretreatment lymphocyte-to-monocyte ratio in patients with urologic tumors: A PRISMA-compliant meta-analysis
Abstract
Background: The prognostic value of pretreatment lymphocyte to monocyte ratio (LMR) in patients with urologic tumors remains controversial. Therefore, we herein conducted a meta-analysis to systematically assess the prognostic value of LMR in patients with urologic tumors.
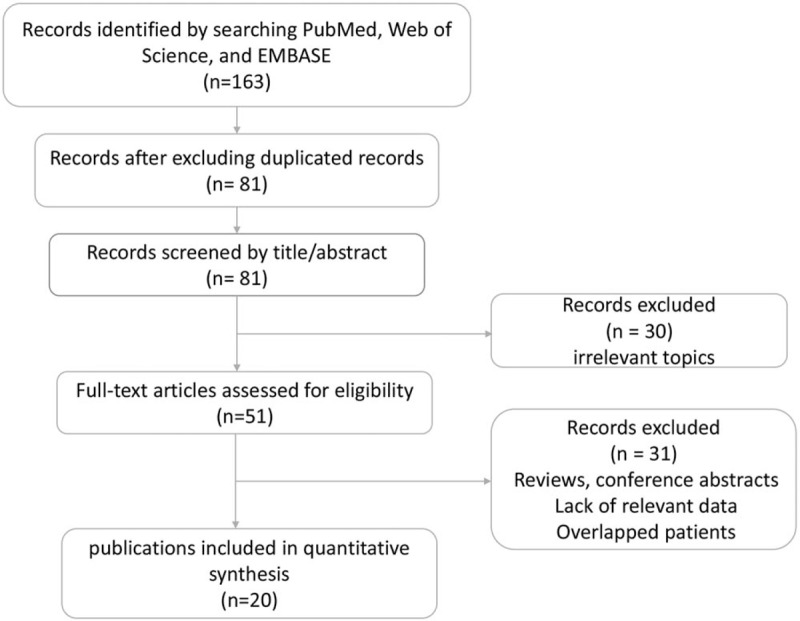
Methods: We comprehensively searched PubMed, EMBASE and Web of Science to identify eligible studies. Hazard ratios (HRs) and their 95% confidence intervals (CIs) were used to assess the prognostic value of LMR in patients with urologic tumors. This meta-analysis was registered in PROSPERO (CRD42018108959).
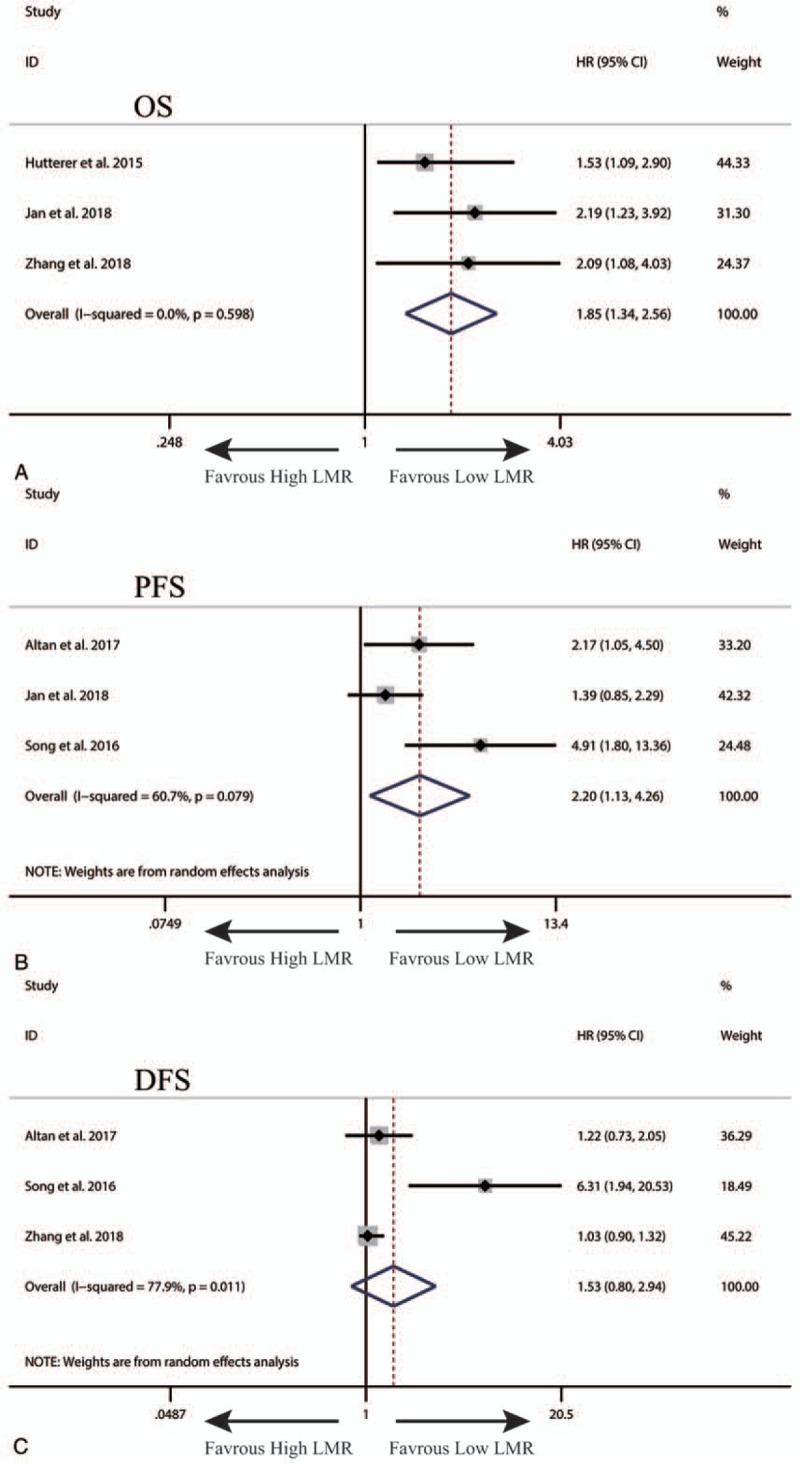
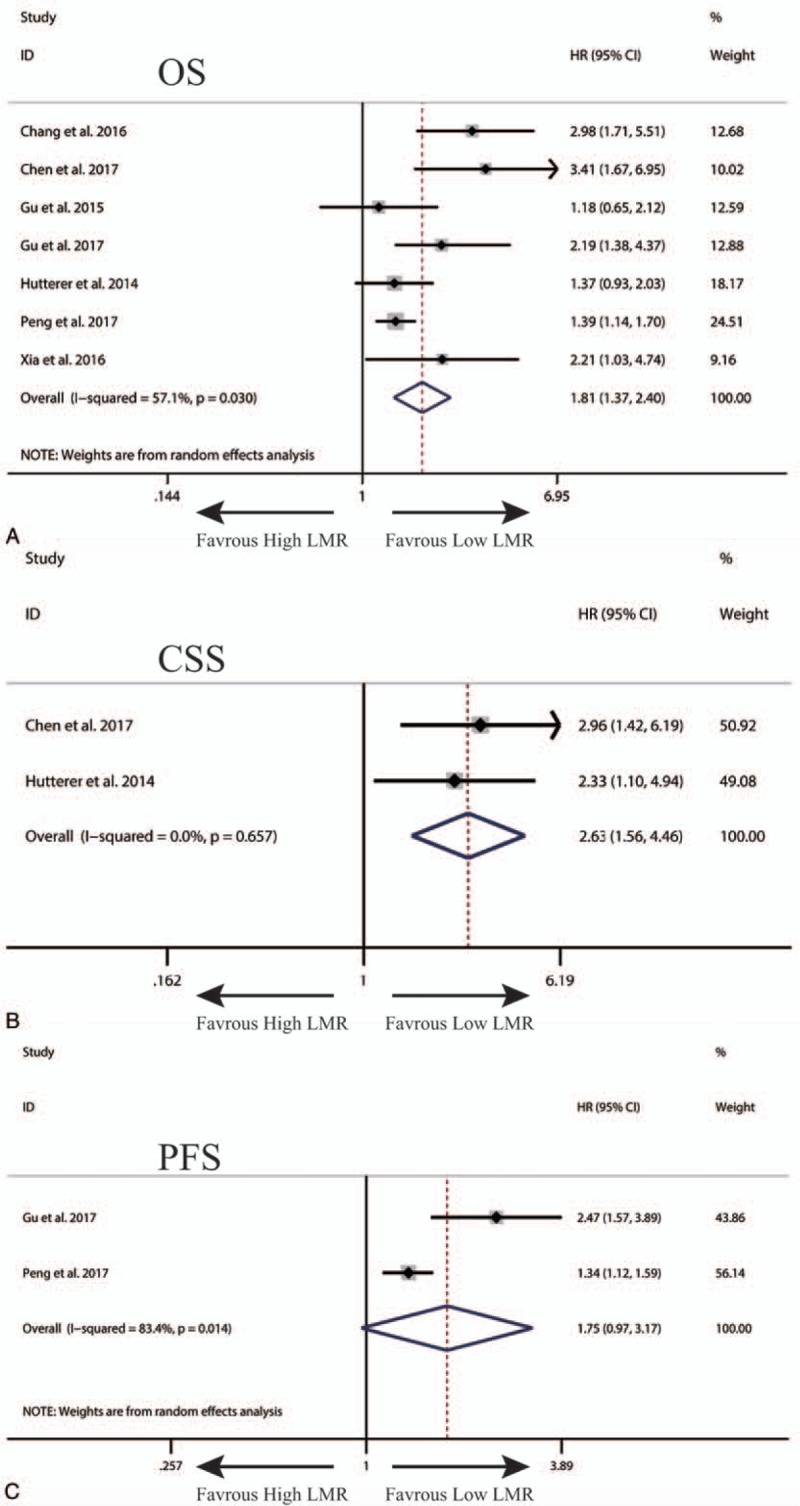
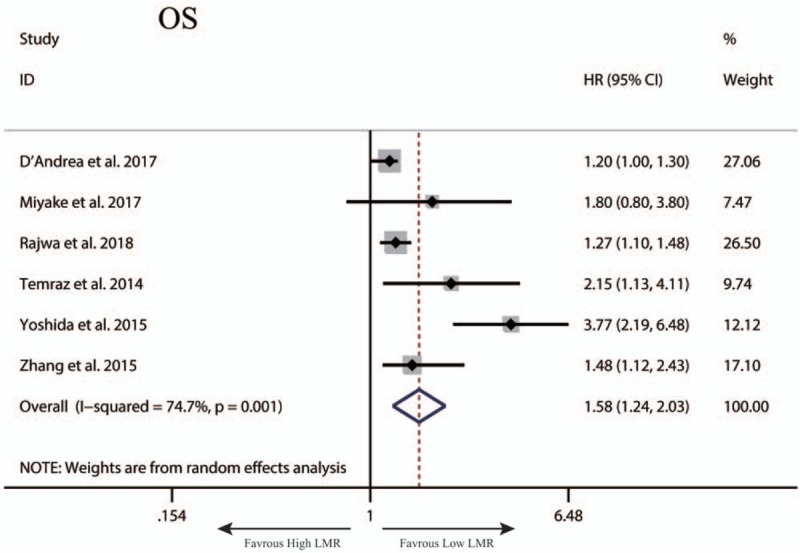
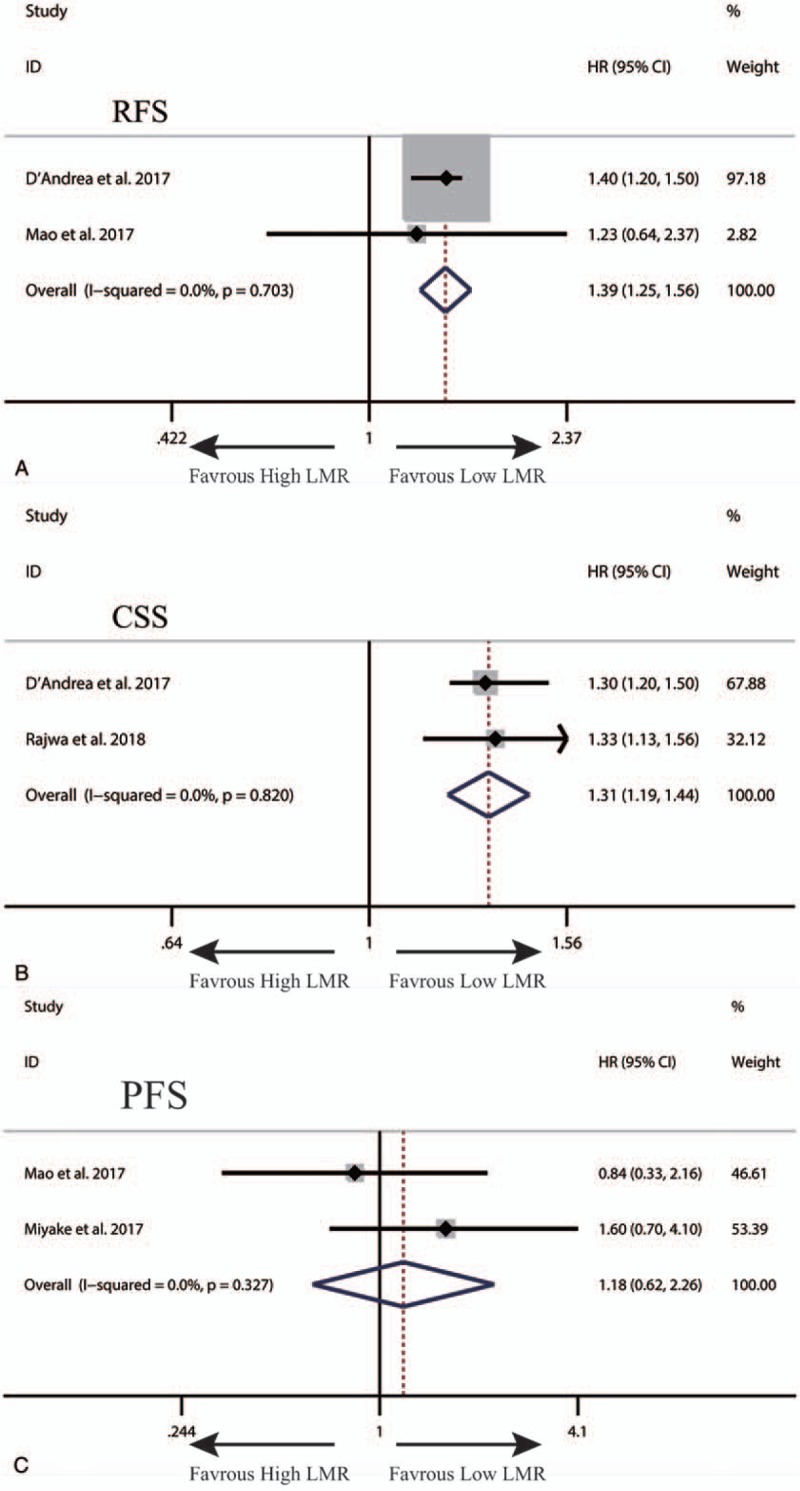
Results: A total of 20 studies were included in this meta-analysis. Our synthesized analysis showed that low LMR was significantly correlated with poor overall survival (OS) and progression-free survival (PFS) in patients with upper tract urothelial cancer (UTUC). We also found that renal cell cancer (RCC) patients with low LMR had poor OS, PFS and cancer-specific survival (CSS). Besides, it was observed that low LMR predicted poor OS, RFS and CSS in patients with bladder cancer (BC).
Conclusion: This meta-analysis demonstrated that pretreatment LMR is associated with survival, and may be a useful prognostic parameter in urologic tumors. Nevertheless, more prospective and heterogeneous studies with large samples are required to further confirm our findings before it is applied for daily clinical decision making.
Conflict of interest statement
All the authors declare no conflicts of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin 2017;67:7–30. - PubMed
-
- Rini BI, Escudier B, Tomczak P, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial. Lancet 2011;378:1931–9. - PubMed
-
- Kimura T, Egawa S, Uemura H. Personalized peptide vaccines and their relation to other therapies in urological cancer. Nat Rev Urol 2017;14:501–10. - PubMed
-
- Mathieu R, Vartolomei MD, Mbeutcha A, et al. Urothelial cancer of the upper urinary tract: emerging biomarkers and integrative models for risk stratification. Minerva Urol Nefrol 2016;68:381–95. - PubMed
-
- Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet 2001;357:539–45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
