

Establishment of vaginal microbiota composition in early pregnancy and its association with subsequent preterm prelabor rupture of the fetal membranes
- PMID: 30633889
- PMCID: PMC6489901
- DOI: 10.1016/j.trsl.2018.12.005
Establishment of vaginal microbiota composition in early pregnancy and its association with subsequent preterm prelabor rupture of the fetal membranes
Abstract
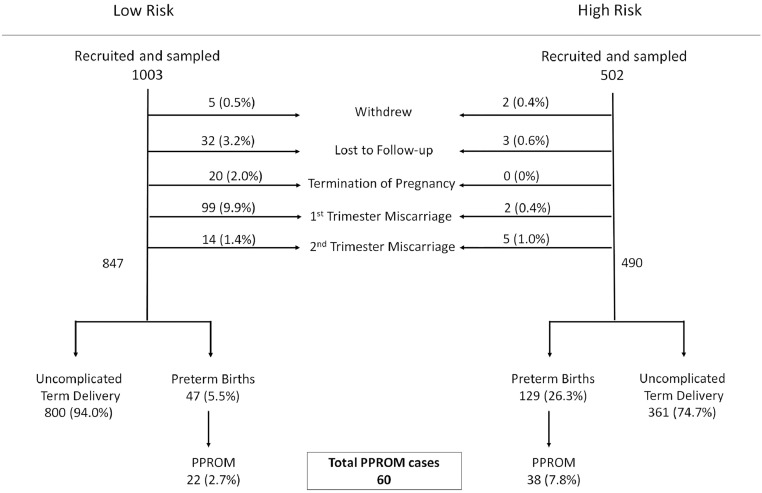
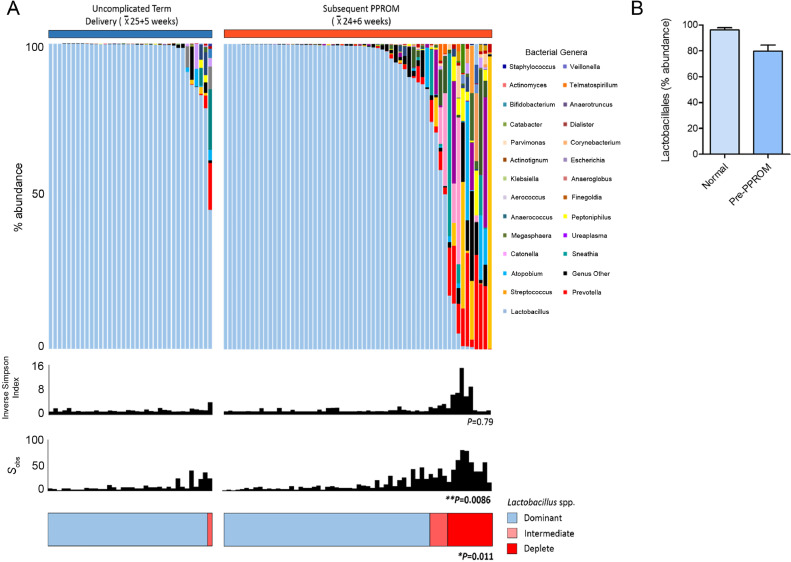
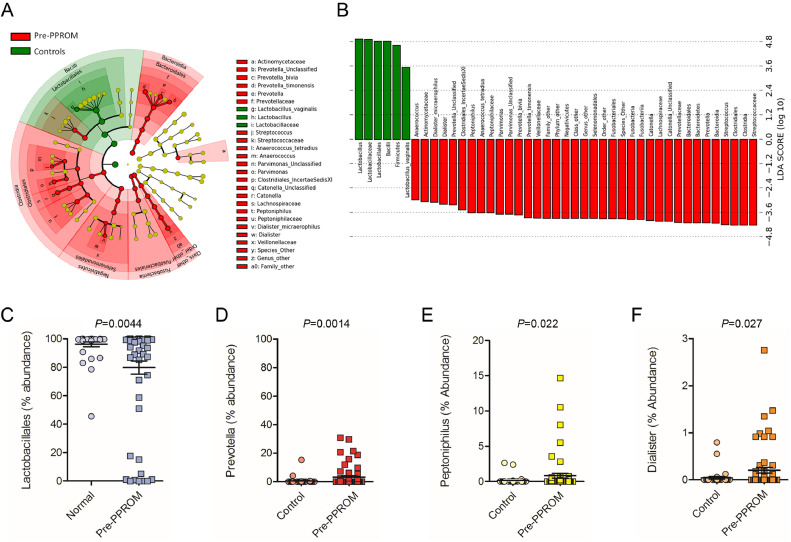
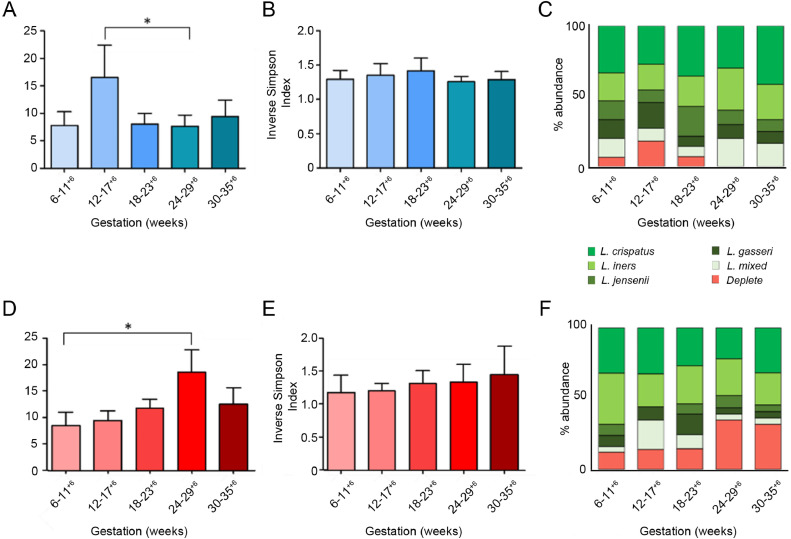
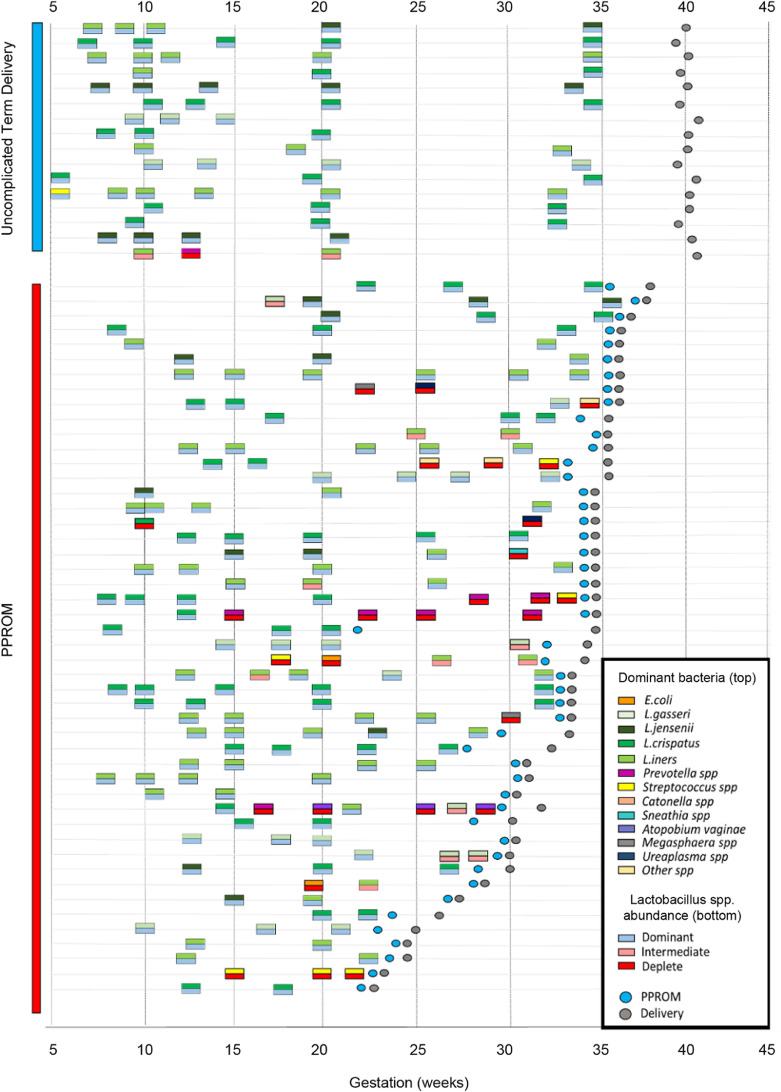
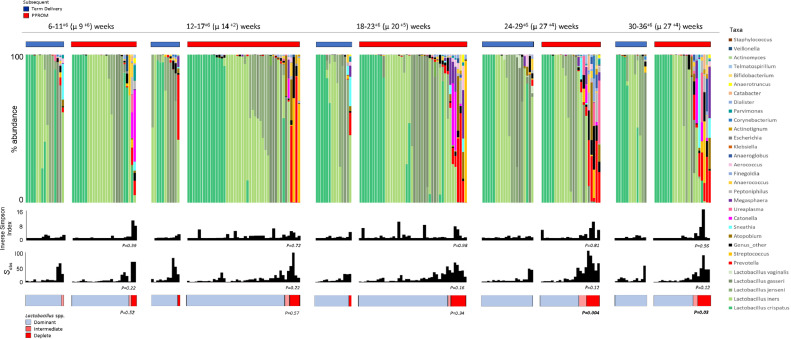
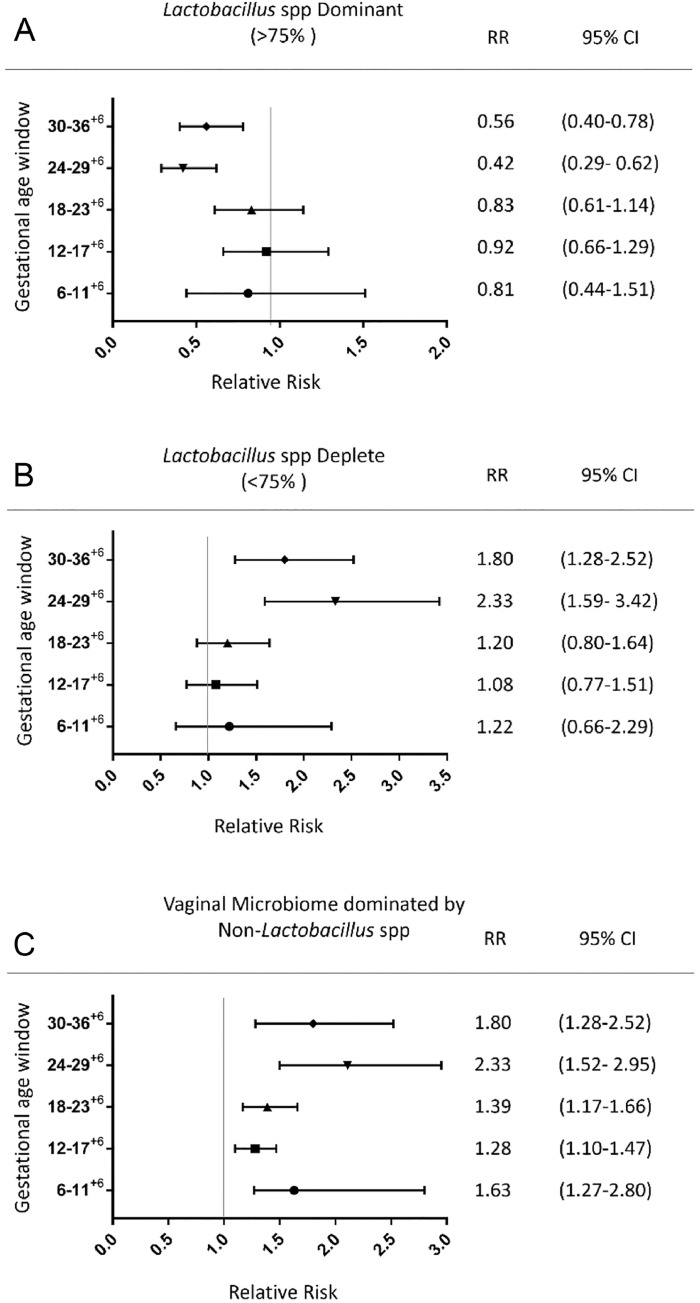
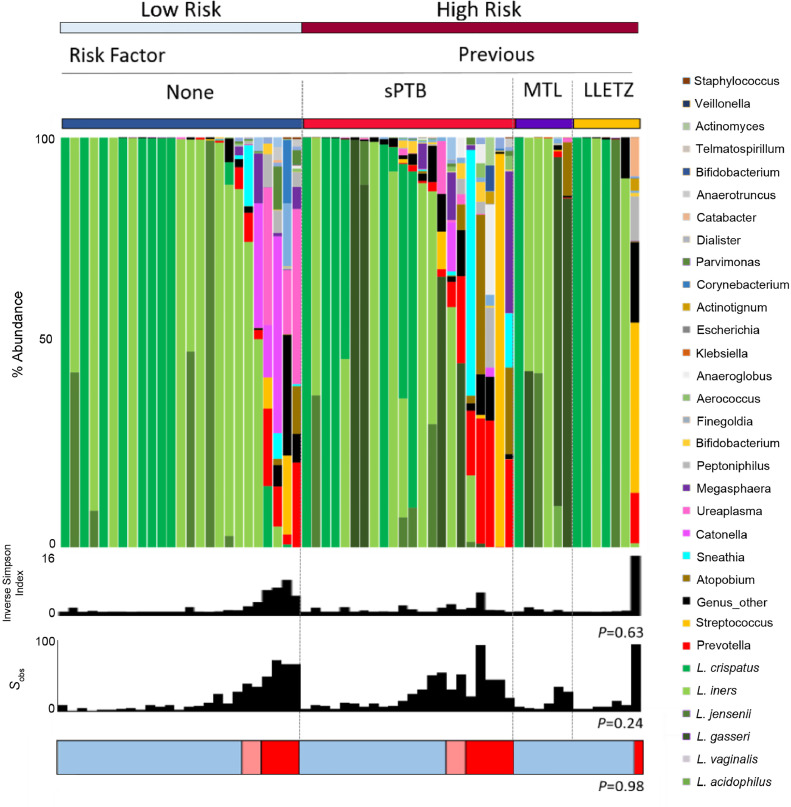
Vaginal bacterial community composition influences pregnancy outcome. Preterm prelabor rupture of the fetal membranes (PPROM), which precedes 30% of all spontaneous preterm births, is associated with high vaginal bacterial diversity prior to rupture. The point at which vaginal bacterial diversity is established before PPROM is unknown. In this study, we use metataxonomics to longitudinally characterize the vaginal bacterial composition from as early as 6 weeks of gestation in women at high (n = 38) and low (n = 22) risk of preterm birth who subsequently experience PPROM and in women delivering at term without complications (n = 36). Reduced Lactobacillus spp. abundance and high diversity was observed prior to PPROM in 20% and 26% of women at low and high risk of preterm births respectively, but in only 3% of women who delivered at term. PPROM was associated with instability of bacterial community structure during pregnancy and a shift toward higher diversity predominately occurring during the second trimester. This was characterized by increased relative abundance of potentially pathogenic species including Prevotella, Peptoniphilus, Streptococcus, and Dialister. This study identifies reduced Lactobacillus spp. abundance and increasing vaginal bacterial diversity as an early risk factor for PPROM and highlights the need for interventional studies designed to assess the impact of modifying vaginal bacterial composition for the prevention of preterm birth.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- WHO, World Health Organisation. Causes of child mortality. In: Global Health Observatory (GHO) Data. 2017. https://www.who.int/gho/child_health/mortality/causes/en/.
-
- Parry S., Strauss J.F., 3rd Premature rupture of the fetal membranes. N Engl J Med. 1998;338:663–670. - PubMed
-
- Liu L., Oza S., Hogan D., Perin J., Rudan I., Lawn J.E. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385:430–440. - PubMed
-
- Chandiramani M., Bennett P.R., Brown R., Lee Y., MacIntyre D.A. Vaginal microbiome-pregnant host interactions determine a significant proportion of preterm labour. Fetal Matern Med Rev. 2014;25:73–78.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
