

Predicting mortality in patients undergoing VA-ECMO after coronary artery bypass grafting: the REMEMBER score
- PMID: 30635022
- PMCID: PMC6330483
- DOI: 10.1186/s13054-019-2307-y
Predicting mortality in patients undergoing VA-ECMO after coronary artery bypass grafting: the REMEMBER score
Abstract
Background: Prediction scoring systems for coronary artery bypass grafting (CABG) patients on venoarterial extracorporeal membrane oxygenation (VA-ECMO) have not yet been reported. This study was designed to develop a predictive score for in-hospital mortality for cardiogenic shock patients who received VA-ECMO after isolated CABG.
Methods: Retrospective cohort study of consecutive CABG patients supported with VA-ECMO (n = 166) at the Beijing Anzhen Hospital between February 2004 and March 2017.
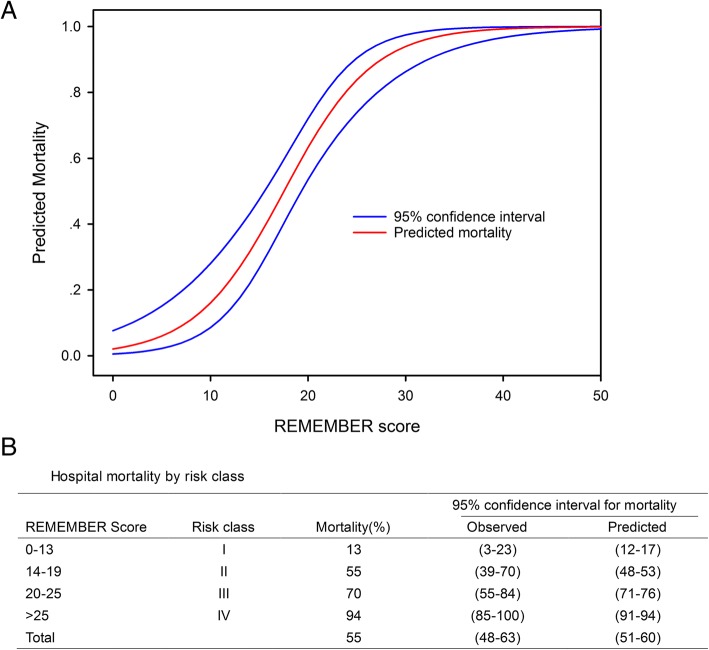
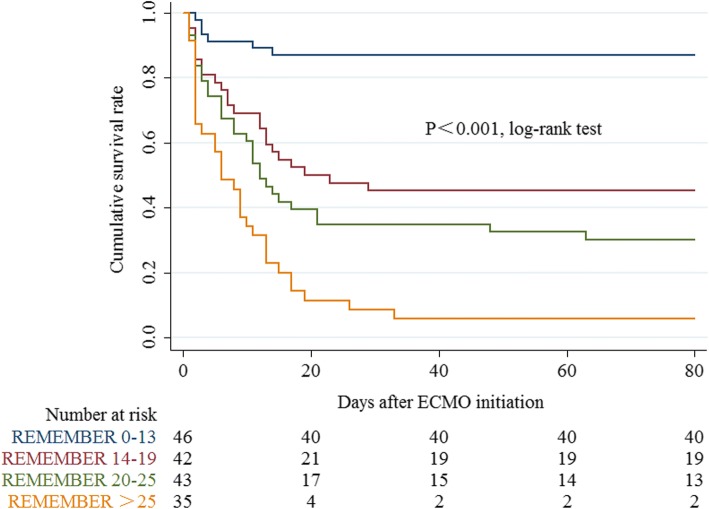
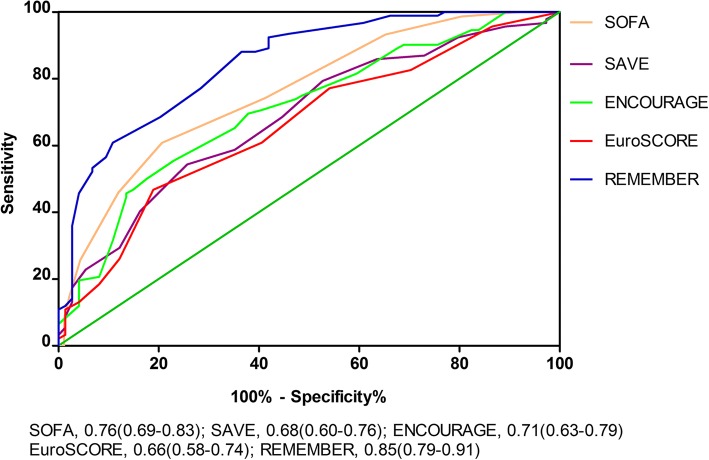
Results: One hundred and six patients (64%) could be weaned from VA-ECMO, and 74 patients (45%) survived to hospital discharge. On the basis of multivariable logistic regression analyses, the pRedicting mortality in patients undergoing veno-arterial Extracorporeal MEMBrane oxygenation after coronary artEry bypass gRafting (REMEMBER) score was created with six pre-ECMO parameters: older age, left main coronary artery disease, inotropic score > 75, CK-MB > 130 IU/L, serum creatinine > 150 umol/L, and platelet count < 100 × 109/L. Four risk classes, namely class I (REMEMBER score 0-13), class II (14-19), class III (20-25), and class IV (> 25) with their corresponding mortality (13%, 55%, 70%, and 94%, respectively), were identified. The area under the receiver operating characteristic curve 0.85(95% CI 0.79-0.91) for the REMEMBER score was better than those for the SOFA, SAVE, EuroSCORE, and ENCOURAGE scores in this population.
Conclusions: The REMEMBER score might help clinicians at bedside to predict in-hospital mortality for patients receiving VA-ECMO after isolated CABG for refractory cardiogenic shock. Prospective studies are needed to externally validate this scoring system.
Keywords: Cardiogenic shock; Coronary artery bypass grafting; Mortality; Venoarterial extracorporeal membrane oxygenation; pRedicting mortality in patients undergoing veno-arterial Extracorporeal MEMBrane oxygenation after coronary artEry bypass gRafting (REMEMBER) score.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the institutional ethics committee/review board of the Beijing Anzhen Hospital. Informed consent for demographic, physiological and hospital-outcome data analyses was not obtained because this observational study did not modify existing diagnostic or therapeutic strategies. However, patients and/or relatives were informed about the anonymous data collection and that they could decline inclusion.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Important methodological flaws in the recently published clinical prediction model the REMEMBER score.Crit Care. 2019 Mar 7;23(1):71. doi: 10.1186/s13054-019-2363-3. Crit Care. 2019. PMID: 30845996 Free PMC article. No abstract available.
-
Short-term assist devices in postcardiotomy cardiogenic shock.Crit Care. 2019 Jun 3;23(1):199. doi: 10.1186/s13054-019-2471-0. Crit Care. 2019. PMID: 31159848 Free PMC article. No abstract available.
-
Predicting mortality after postcardiotomy venoarterial extracorporeal membrane oxygenation.Ann Transl Med. 2019 Jul;7(Suppl 3):S100. doi: 10.21037/atm.2019.04.74. Ann Transl Med. 2019. PMID: 31576307 Free PMC article. No abstract available.
References
-
- Rastan AJ, Dege A, Mohr M, Doll N, Falk V, Walther T, et al. Early and late outcomes of 517 consecutive adult patients treated with extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. J Thorac Cardiovasc Surg. 2010;139:302–311. doi: 10.1016/j.jtcvs.2009.10.043. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
