

Telomere length and genetic variant associations with interstitial lung disease progression and survival
- PMID: 30635297
- PMCID: PMC6612265
- DOI: 10.1183/13993003.01641-2018
Telomere length and genetic variant associations with interstitial lung disease progression and survival
Abstract
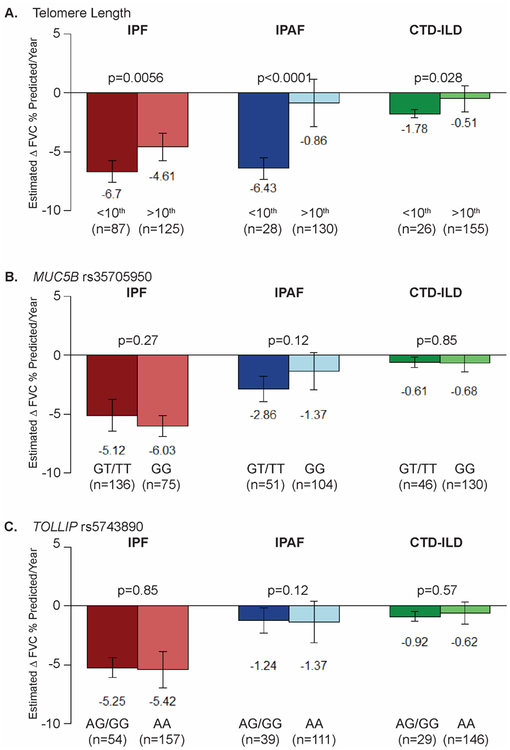
Leukocyte telomere length (LTL), MUC5B rs35705950 and TOLLIP rs5743890 have been associated with idiopathic pulmonary fibrosis (IPF).In this observational cohort study, we assessed the associations between these genomic markers and outcomes of survival and rate of disease progression in patients with interstitial pneumonia with autoimmune features (IPAF, n=250) and connective tissue disease-associated interstitial lung disease (CTD-ILD, n=248). IPF (n=499) was used as a comparator.The LTL of IPAF and CTD-ILD patients (mean age-adjusted log-transformed T/S of -0.05±0.29 and -0.04±0.25, respectively) is longer than that of IPF patients (-0.17±0.32). For IPAF patients, LTL <10th percentile is associated with faster lung function decline compared to LTL ≥10th percentile (-6.43% per year versus -0.86% per year; p<0.0001) and worse transplant-free survival (hazard ratio 2.97, 95% CI 1.70-5.20; p=0.00014). The MUC5B rs35705950 minor allele frequency (MAF) is greater for IPAF patients (23.2, 95% CI 18.8-28.2; p<0.0001) than controls and is associated with worse transplant-free IPAF survival (hazard ratio 1.92, 95% CI 1.18-3.13; p=0.0091). Rheumatoid arthritis (RA)-associated ILD (RA-ILD) has a shorter LTL than non-RA CTD-ILD (-0.14±0.27 versus -0.01±0.23; p=0.00055) and higher MUC5B MAF (34.6, 95% CI 24.4-46.3 versus 14.1, 95% CI 9.8-20.0; p=0.00025). Neither LTL nor MUC5B are associated with transplant-free CTD-ILD survival.LTL and MUC5B MAF have different associations with lung function progression and survival for IPAF and CTD-ILD.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: C.A. Newton reports grants from the National Institutes of Health (KL2TR001103), during the conduct of the study. Conflict of interest: J.M. Oldham reports grants from the National Heart, Lung, and Blood Institute (NHLBI), and personal fees from Genentech and Boehringer Ingelheim, outside the submitted work. Conflict of interest: B. Ley has nothing to disclose. Conflict of interest: V. Anand has nothing to disclose. Conflict of interest: A. Adegunsoye reports speaking fees and honoraria for advisory boards with Boehringer Ingelheim related to idiopathic pulmonary fibrosis (IPF) within the last 12 months. Conflict of interest: G. Liu has nothing to disclose. Conflict of interest: K. Batra has nothing to disclose. Conflict of interest: J. Torrealba reports personal fees for expert panel work from Roche–Ventana and AbbVie, outside the submitted work. Conflict of interest: J. Kozlitina has nothing to disclose. Conflict of interest: C. Glazer is a member of a speaker bureau for Genentech. There is no discussion of therapy in this paper. Conflict of interest: M.E. Strek reports grants and personal fees for advisory board work and speaker fees from Boehringer Ingelheim, and grants from Genentech-Roche, Gilead and MedImmune, outside the submitted work. Conflict of interest: P.J. Wolters reports grants from Medimmune and Genentech, and personal fees from Roche and Boehringer Ingelheim, outside the submitted work. Conflict of interest: I. Noth reports personal fees for consultancy from Boehringer Ingelheim, Genentech, Sanofi Aventis and Global Blood Therapeutics, outside the submitted work, and has a patent pending on TOLLIP and IPF pharmacogenomics. Conflict of interest: C.K. Garcia reports grants from the National Institutes of Health (R01 HL09309) during the conduct of the study and was previously a member of the advisory board for Pliant Therapeutics.
Figures
Comment in
-
Advances in Interstitial Lung Disease Genetics.Am J Respir Crit Care Med. 2019 Jul 15;200(2):247-249. doi: 10.1164/rccm.201902-0471RR. Am J Respir Crit Care Med. 2019. PMID: 31014082 No abstract available.