

Rheumatoid arthritis presenting as rheumatoid meningitis
- PMID: 30635304
- PMCID: PMC6340586
- DOI: 10.1136/bcr-2018-226649
Rheumatoid arthritis presenting as rheumatoid meningitis
Abstract
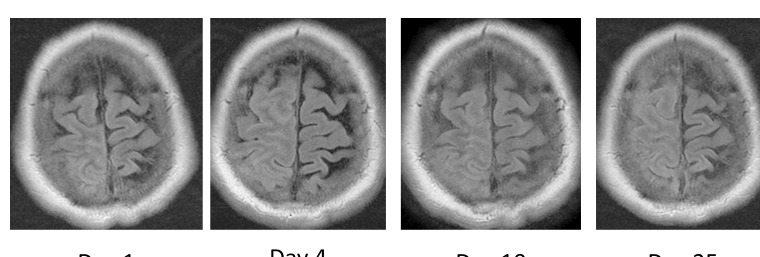
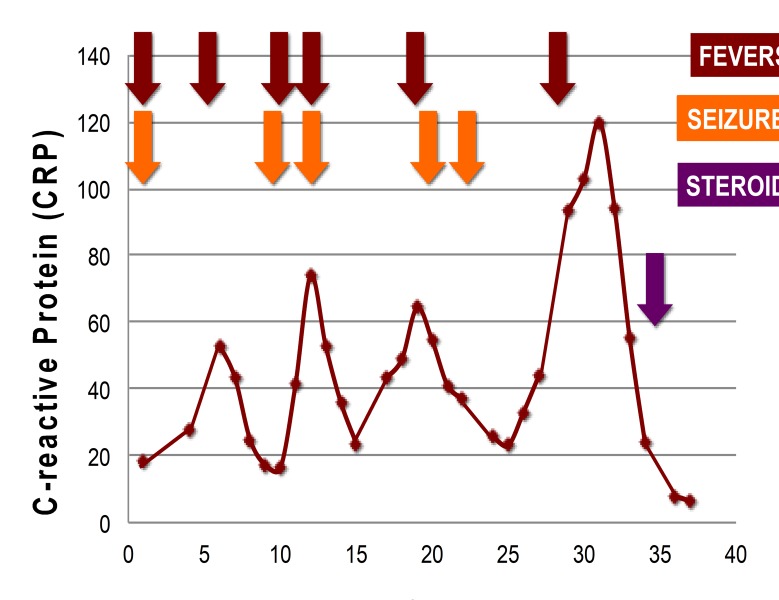
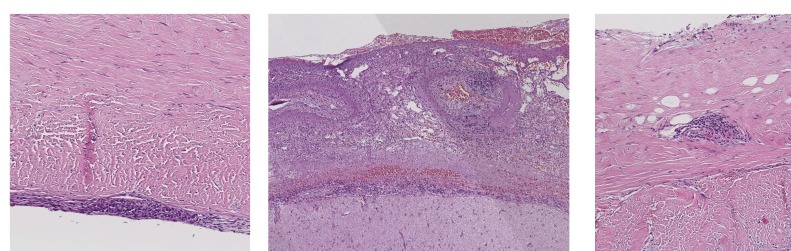
Rheumatoid meningitis (RM) is a rare extra-articular manifestation of rheumatoid arthritis (RA). A 59-year-old man presented with a 10-day history of right-sided frontal headache and a 7-day history of subacute left-sided weakness. He had no history of RA. He was febrile (38.2°C). Left ankle dorsiflexion and plantarflexion were graded at 4+/5. He developed focal onset motor seizures. He was intermittently febrile with minimal improvement despite intravenous antivirals and antimicrobials. Serology revealed elevated rheumatoid factor 88.2 IU/mL and anti-cyclic citrullinated peptide (anti-CCP) IgG >340 AU/mL. Initial cerebrospinal fluid (CSF) was predominantly lymphocytic 96%, with elevated protein 672 mg/L and normal glucose 3.4 mmol/L. Interval CSF revealed newly low glucose 2.6 mmol/L. Extensive CSF microbiology tests were negative. CSF cytology confirmed reactive lymphocytes. MRI brain revealed right frontoparietal leptomeningeal enhancement. Brain and leptomeningeal biopsy demonstrated florid leptomeningeal mixed inflammatory infiltrate without granulomas. The combination of elevated anti-CCP IgG, erosive arthropathy, CSF lymphocytosis, asymmetrical leptomeningeal enhancement and biopsy findings confirmed RM.
Keywords: headache (including migraines); meningitis; rheumatoid arthritis.
© BMJ Publishing Group Limited 2019. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical