

TP53 mutation status divides myelodysplastic syndromes with complex karyotypes into distinct prognostic subgroups
- PMID: 30635634
- PMCID: PMC6609480
- DOI: 10.1038/s41375-018-0351-2
TP53 mutation status divides myelodysplastic syndromes with complex karyotypes into distinct prognostic subgroups
Abstract
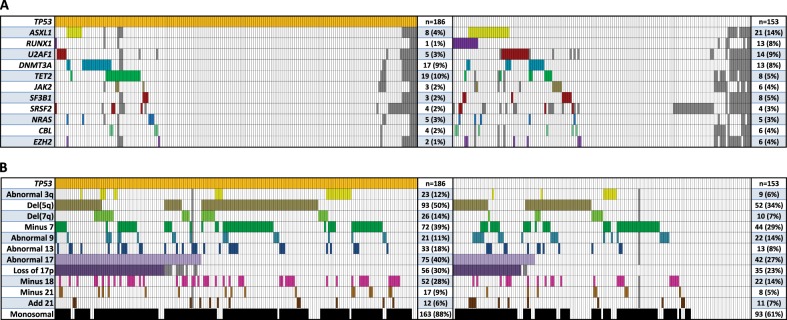
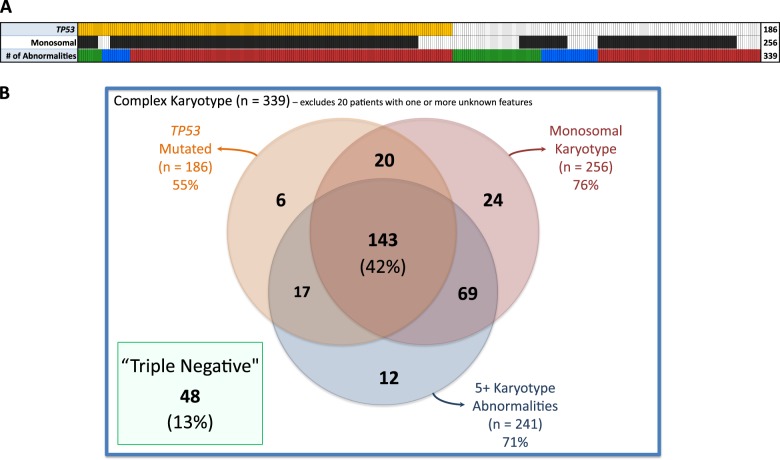
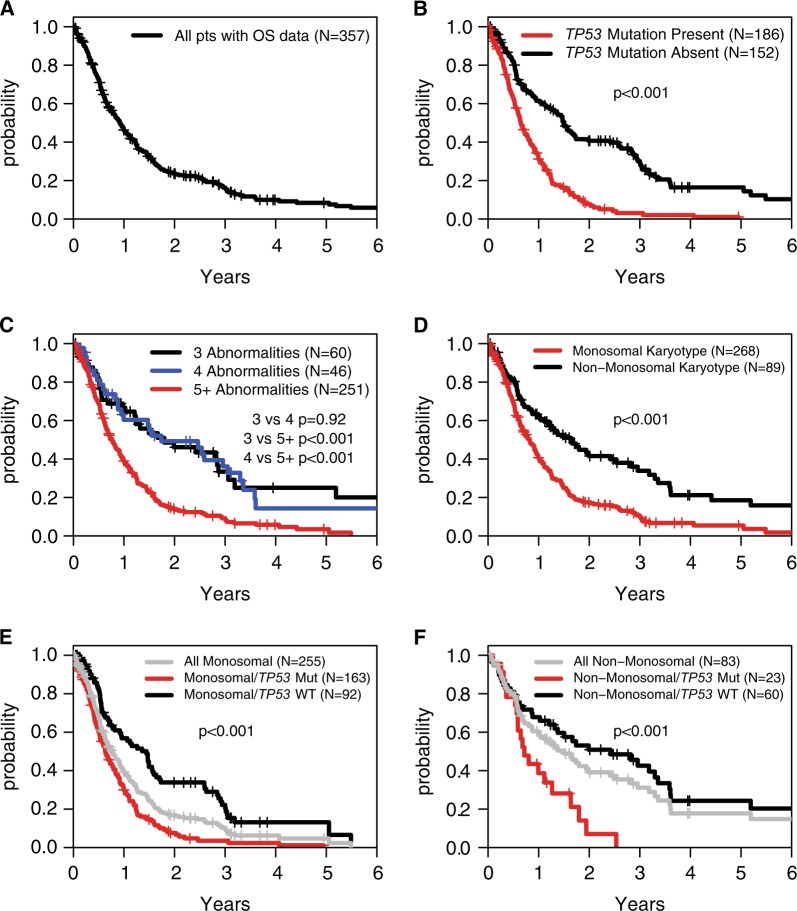
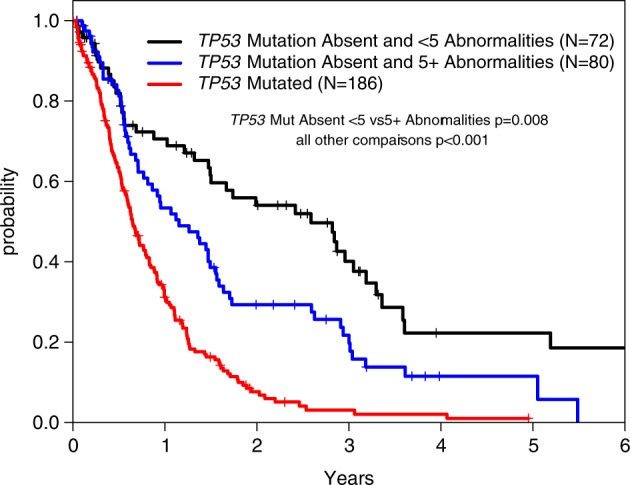
Risk stratification is critical in the care of patients with myelodysplastic syndromes (MDS). Approximately 10% have a complex karyotype (CK), defined as more than two cytogenetic abnormalities, which is a highly adverse prognostic marker. However, CK-MDS can carry a wide range of chromosomal abnormalities and somatic mutations. To refine risk stratification of CK-MDS patients, we examined data from 359 CK-MDS patients shared by the International Working Group for MDS. Mutations were underrepresented with the exception of TP53 mutations, identified in 55% of patients. TP53 mutated patients had even fewer co-mutated genes but were enriched for the del(5q) chromosomal abnormality (p < 0.005), monosomal karyotype (p < 0.001), and high complexity, defined as more than 4 cytogenetic abnormalities (p < 0.001). Monosomal karyotype, high complexity, and TP53 mutation were individually associated with shorter overall survival, but monosomal status was not significant in a multivariable model. Multivariable survival modeling identified severe anemia (hemoglobin < 8.0 g/dL), NRAS mutation, SF3B1 mutation, TP53 mutation, elevated blast percentage (>10%), abnormal 3q, abnormal 9, and monosomy 7 as having the greatest survival risk. The poor risk associated with CK-MDS is driven by its association with prognostically adverse TP53 mutations and can be refined by considering clinical and karyotype features.
Conflict of interest statement
RB has served as a consultant for Genoptix and Celgene and served on advisory boards for Otsuka/Astex, AbbVie/Genetech, and Celgene and has received research funding from Celgene and Takeda. DH has served as consultant and advisory board member for Celgene and Novartis from both of which he has received research funding. PV receives research funding from Celgene and has been on advisory boards for Celgene, Pfizer, Novartis, Jazz, Daiichi Sanko. LQ receives research funding from Celgene. MAS has served on an advisory board for Celgene. MRE reports consultancy and research funding from Astex, Incyte, Karyopharm, Sunesis, Takeda, and TG Therapeutics; equity in Karyopharm; and DSMB membership for Celgene and Gilead. TH, CH, and WK report partial ownership of MLL–Munich Leukemia Laboratory. All other authors declare that they have no conflict of interest.
Figures
References
-
- Schanz J, Tuchler H, Sole F, et al. New comprehensive cytogenetic scoring system for primary myelodysplastic syndromes (MDS) and oligoblastic acute myeloid leukemia after MDS derived from an international database merge. J Clin Oncol. 2012;30:820–9. doi: 10.1200/JCO.2011.35.6394. - DOI - PMC - PubMed
-
- Schanz J, Steidl C, Fonatsch C, et al. Coalesced multicentric analysis of 2,351 patients with myelodysplastic syndromes indicates an underestimation of poor-risk cytogenetics of myelodysplastic syndromes in the international prognostic scoring system. J Clin Oncol. 2011;29:1963–70. doi: 10.1200/JCO.2010.28.3978. - DOI - PMC - PubMed
-
- Greenberg P, Cox C, LeBeau MM, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89:2079–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50 CA206963/CA/NCI NIH HHS/United States
- MC_UU_00016/11/MRC_/Medical Research Council/United Kingdom
- K12 CA076917/CA/NCI NIH HHS/United States
- MC_UU_12009/11/MRC_/Medical Research Council/United Kingdom
- P30 CA008748/CA/NCI NIH HHS/United States
- MC_U137961146/MRC_/Medical Research Council/United Kingdom
- G1000729/94931/MRC_/Medical Research Council/United Kingdom
- P01 CA101937/CA/NCI NIH HHS/United States
- K08 DK091360/DK/NIDDK NIH HHS/United States
- MR/R007608/1/MRC_/Medical Research Council/United Kingdom
- MR/L008963/1/MRC_/Medical Research Council/United Kingdom
- G1000729/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
