

The Relationships Between Time in Range, Hyperglycemia Metrics, and HbA1c
- PMID: 30636519
- PMCID: PMC6610606
- DOI: 10.1177/1932296818822496
The Relationships Between Time in Range, Hyperglycemia Metrics, and HbA1c
Abstract
Background: As the use of continuous glucose monitoring (CGM) increases, there is a need to better understand key metrics of time in range 70-180 mg/dL (TIR70-180) and hyperglycemia and how they relate to hemoglobin A1c (A1C).
Methods: Analyses were conducted utilizing datasets from four randomized trials encompassing 545 adults with type 1 diabetes (T1D) who had central-laboratory measurements of A1C. CGM metrics were calculated and compared with each other and A1C cross-sectionally and longitudinally.
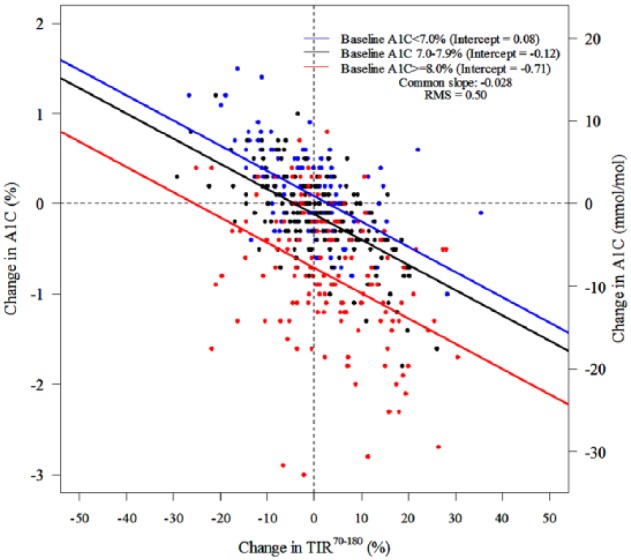
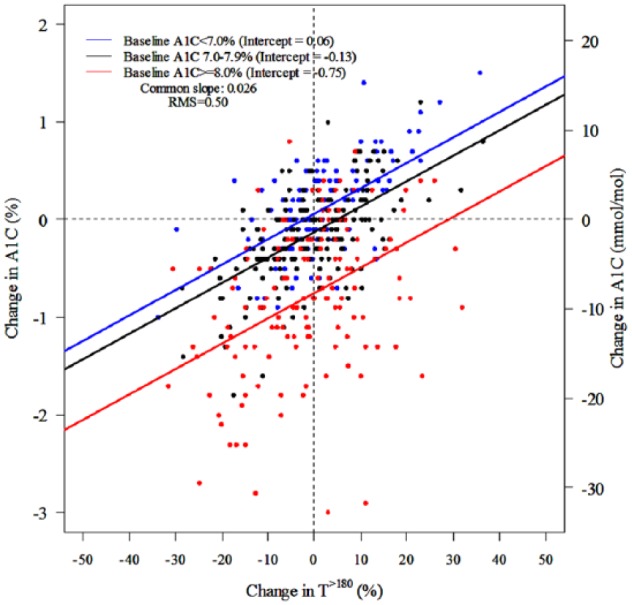
Results: Correlations among CGM metrics (TIR70-180, time >180 mg/dL, time >250 mg/dL, mean glucose, area under the curve above 180 mg/dL, high blood glucose index, and time in range 70-140 mg/dL) were typically 0.90 or greater. Correlations of each metric with A1C were lower (absolute values 0.66-0.71 at baseline and 0.73-0.78 at month 6). For a given TIR70-180 percentage, there was a wide range of possible A1C levels that could be associated with that TIR70-180 level. On average, a TIR70-180 of 70% and 50% corresponded with an A1C of approximately 7% and 8%, respectively. There also was considerable spread of change in A1C for a given change in TIR70-180, and vice versa. An increase in TIR70-180 of 10% (2.4 hours per day) corresponded to a decrease in A1C of 0.6%, on average.
Conclusions: In T1D, CGM measures reflecting hyperglycemia (including TIR and mean glucose) are highly correlated with each other but only moderately correlated with A1C. For a given TIR or change in TIR there is a wide range of possible corresponding A1C values.
Keywords: continuous glucose monitoring; glucose time in range; type 1 diabetes.
Conflict of interest statement
Figures

Comment in
-
Interpreting the recent consensus on time in range for interstitial glucose right - Or wrong?Diabetes Res Clin Pract. 2020 Apr;162:108106. doi: 10.1016/j.diabres.2020.108106. Epub 2020 Mar 12. Diabetes Res Clin Pract. 2020. PMID: 32173416 No abstract available.
References
-
- Yudkin JS, Forrest RD, Jackson CA, Ryle AJ, Davie S, Gould BJ. Unexplained variability of glycated haemoglobin in non-diabetic subjects not related to glycaemia. Diabetologia. 1990;33:208-215. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
