

Ethnic disparity in Israel impacts long-term results after heart transplantation
- PMID: 30636628
- PMCID: PMC6330742
- DOI: 10.1186/s13584-018-0271-7
Ethnic disparity in Israel impacts long-term results after heart transplantation
Abstract
Background: Ethnicity may affect graft longevity and recipient mortality after heart transplantation (HTx). We hypothesized that differences in ethnic origin between Arabs and Jews undergoing HTx in Israel may contribute to differences in long-term outcomes.
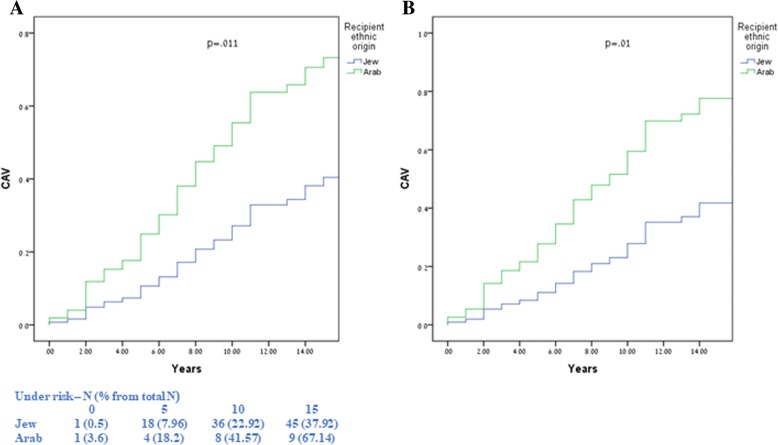
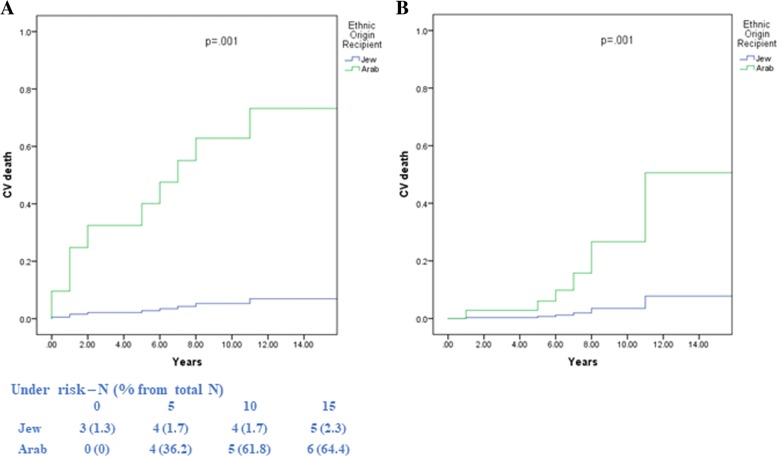
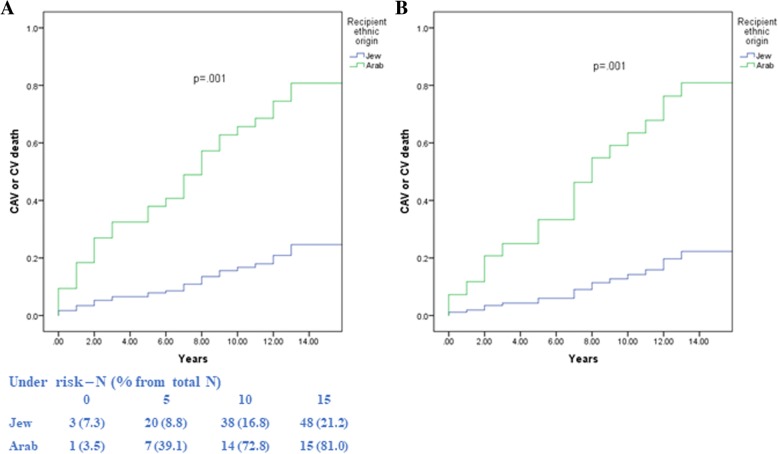
Methods: The study population comprised all 254 patients who underwent HTx between 1991 and 2017 in a tertiary medical center located in the center of Israel. Patients were categorized as either Jews (226 patients, 89%) or Arabs (28 patients, 11%). The primary end point was cardiac allograft vasculopathy (CAV), secondary end points were cardiovascular (CV) mortality and the combined end point of CAV/CV mortality.
Results: In comparison with Jews, Arab patients were significantly younger (ave. age 42 vs. 50) and had shorter in-hospital stay (45 vs. 80 days). However, Kaplan-Meier survival analysis showed that at 10 years of follow-up CAV rates were significantly higher among Arabs (58%) compared with Jews (23%; log-rank P = 0.01) for the overall difference during follow-up. Similar results were shown for the separate end point of CV mortality and the combined end point of CAV/CV mortality. Multivariate analysis, which controlled for age, gender, statin treatment, and other potential confounders, showed that Arab recipient ethnic origin was associated with a significant > 2.5-fold (p = 0.01) increase in the risk for CAV; a > 4-fold increase in the risk for CV mortality (p = 0.001); and approximately 4-fold increase in the risk for the combined end point (p = 0.001). These findings were validated by propensity score analysis.
Conclusions: Our data suggest that Arab ethnic origin is associated with a significantly increased risk for CAV and mortality following HTx. Suggested explanations contributing to ethnic disparities in Israel include socioeconomic, environmental and genetic factors. Further studies are required to evaluate whether more aggressive risk factor management in the Israeli Arab population following HTx would reduce CAV and CV mortality in this high-risk population. Increased awareness and early intervention of the Israeli healthcare system and cooperation with the Arab community is of paramount importance.
Keywords: Arabs; Cardiac allograft vasculopathy; Cardiovascular mortality; Ethnicity; Heart transplantation; Jews.
Conflict of interest statement
Ethics approval and consent to participate
We do declare that the present study was ethically approved by the ethic committee of Sheba Medical Center.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Ethnic disparities in cardiac transplantation: opportunities to improve long-term outcomes in all cardiac transplant recipients.Isr J Health Policy Res. 2019 Jun 11;8(1):53. doi: 10.1186/s13584-019-0320-x. Isr J Health Policy Res. 2019. PMID: 31186060 Free PMC article.
References
-
- Barnard CN. The operation. A human cardiac transplant: an interim report of a successful operation performed at Groote Schuur hospital, Cape Town. S Afr Med J. 1967;41:1271–1274. - PubMed
-
- Lund LH, Khush KK, Cherikh WS, et al. The registry of the International Society for Heart and Lung Transplantation: thirty-fourth adult heart transplantation Report-2017; focus theme: allograft ischemic time. J Heart Lung Transplant. 2017;36:1037–1046. doi: 10.1016/j.healun.2017.07.019. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
