

A Case of Pregnancy Complicated by Primary Hyperparathyroidism Due to a Parathyroid Adenoma
- PMID: 30636767
- PMCID: PMC6340266
- DOI: 10.12659/AJCR.912436
A Case of Pregnancy Complicated by Primary Hyperparathyroidism Due to a Parathyroid Adenoma
Abstract
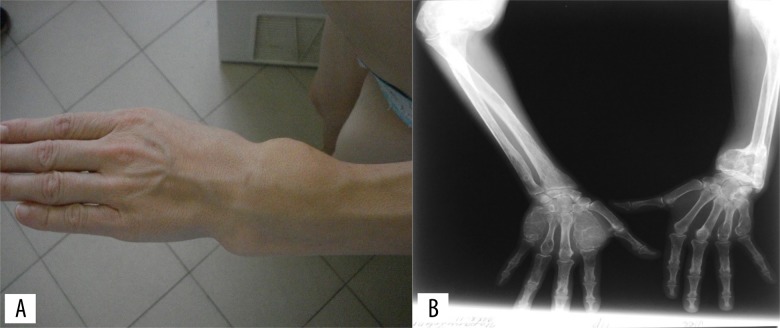
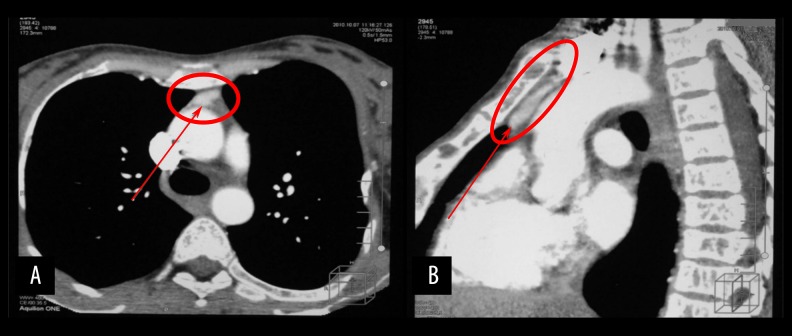
BACKGROUND Primary hyperparathyroidism is most common in women during the menopause and its occurrence in pregnant women is rare. However, because neonatal mortality is associated with maternal hyperparathyroidism, early diagnosis is essential. This report describes the case of a late diagnosis of primary hyperparathyroidism in a 28-year-old pregnant woman and describes the effects on the mother and neonate. CASE REPORT During her second pregnancy, a 28-year-old woman presented with symptoms of general weakness, bone and joint pain, multiple fractures with bone deformity, muscle weakness, and gait disturbance. Due to the high risk of perinatal pathology, a cesarean section was performed. Several weeks later, she underwent thoracoscopic removal of an ectopic parathyroid gland located at the aortic arch. Hypocalcemia in the newborn infant required treatment with calcium and magnesium supplements. CONCLUSIONS This case demonstrates that primary hyperparathyroidism during pregnancy requires timely diagnosis and treatment to reduce potential maternal and fetal complications. Screening for primary hyperparathyroidism should be undertaken in pregnant women with any symptoms associated with hypercalcemia. Treatment should be individualized and includes conservative management, parathyroidectomy in the second trimester, or parathyroidectomy performed in the early postpartum period.
Conflict of interest statement
None.
Figures

References
-
- Schnatz PF, Curry SL. Primary hyperparathyroidism in pregnancy: Evidence-based management. Obstet Gynecol Surv. 2002;57(6):365–76. - PubMed
-
- Tollin SR. Course and outcome of pregnancy in a patient with mild, asymptomatic, primary hyperparathyroidism diagnosed before conception. Am J Med Sci. 2000;320(2):144–47. - PubMed
-
- Dahlman T, Sjöberg HE, Bucht E. Calcium homeostasis in normal pregnancy and puerperium. A longitudinal study. Acta Obstet Gynecol Scand. 1994;73(5):393–98. - PubMed
-
- Breslau NA, Zerwekh JE. Relationship of estrogen and pregnancy to calcium homeostasis in pseudohypoparathyroidism. J Clin Endocrinol Metab. 1986;61(1):45–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
