

Aliphatic Halogenated Hydrocarbons: Report and Analysis of Liver Injury in 60 Patients
- PMID: 30637211
- PMCID: PMC6328725
- DOI: 10.14218/JCTH.2018.00040
Aliphatic Halogenated Hydrocarbons: Report and Analysis of Liver Injury in 60 Patients
Abstract
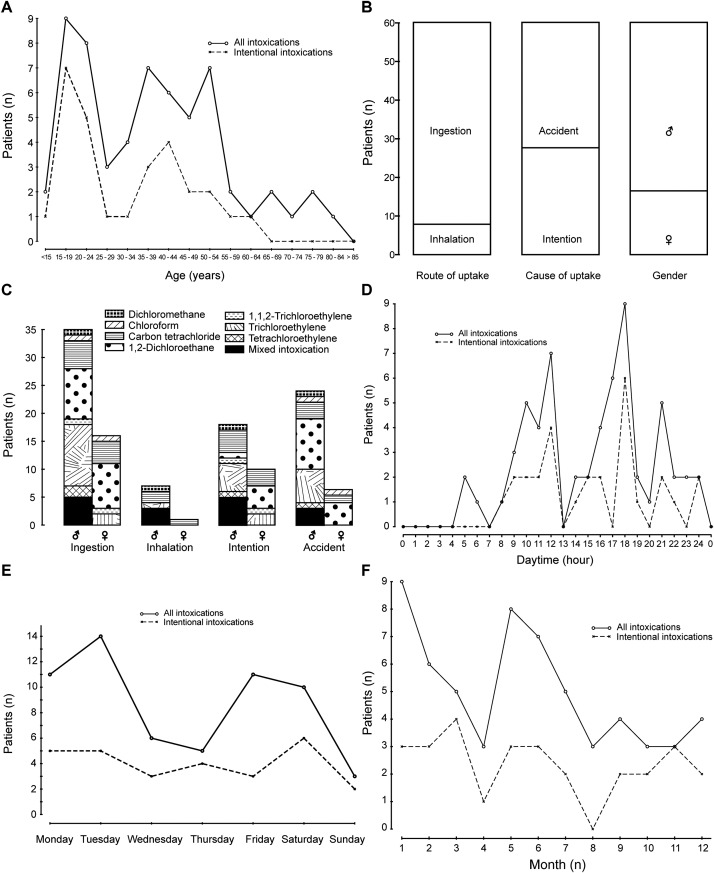
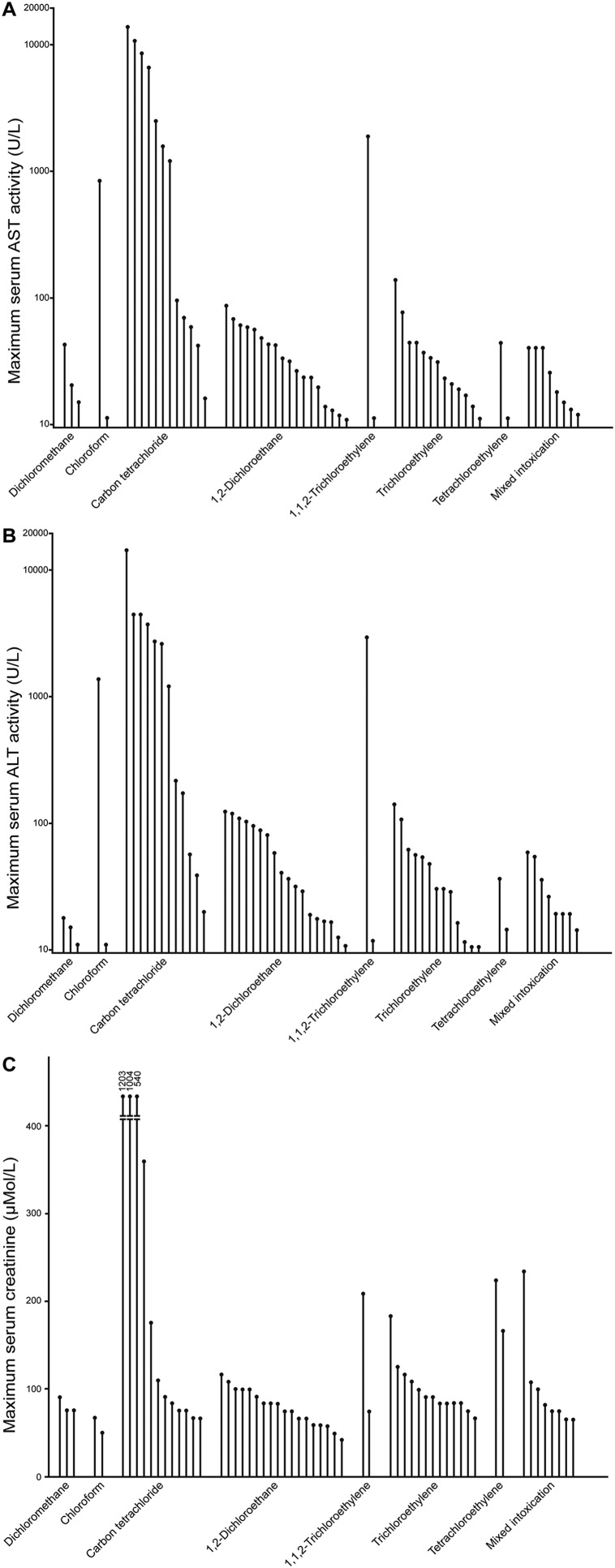
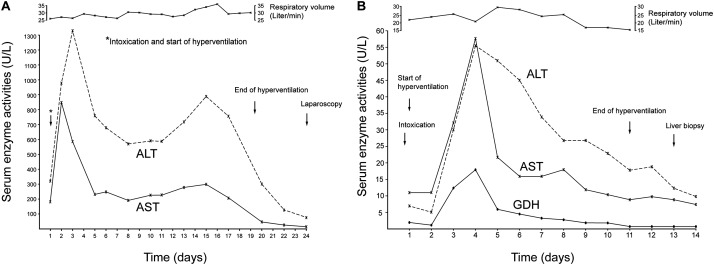
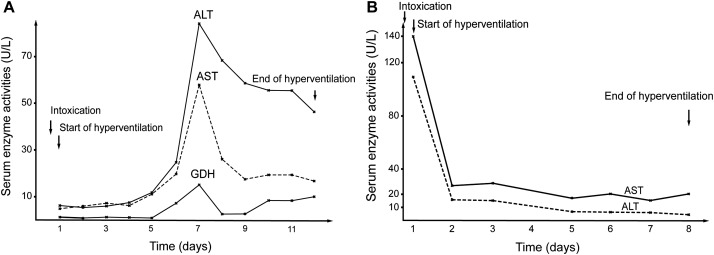
Background and Aims: Intoxications by aliphatic halogenated hydrocarbons (AHH), used as effective solvents, are rare and may cause life-threatening liver injury. Patients with acute intoxications by AHH received an innovative treatment. Methods: Analyzed were data of 60 patients intoxicated by AHH, such as dichloromethane (n = 3), chloroform (n = 2), carbon tetrachloride (n = 12), 1,2-dichloroethane (n = 18), 1,1,2-trichloroethane (n = 2), trichloroethylene (n = 2), tetrachloroethylene (n = 13) or mixed AHH chemicals (n = 8), who received a new treatment consisting of CO2-induced hyperventilation to accelerate toxin removal via the lungs. Results: Added to the inspiration air at a flow rate of 2-3 Liter min-1, CO2 increased the respiratory volume up to 25-30 Liter min-1, ensuring forced AHH exhalation. This CO2-induced hyperventilation therapy was commonly well tolerated by the 60 patients and lasted for 106.0±10.5 hours. In most cases, initially increased liver test results of aminotransferases normalized quickly under the therapy, and liver histology obtained at completion of the therapy revealed, in the majority of patients, normal findings or fatty changes, and rarely severe single cell necrosis but no confluent liver cell necrosis. Despite therapy, clinical outcome was unfavorable for 4/60 patients (6.7%) of the study cohort, due to single or combined risk factors. These included late initiation of the CO2-induced hyperventilation therapy, intentional intoxication, uptake of high amounts of AHH, concomitant ingestion of overdosed drugs, consumption of high amounts of alcohol, and history of alcohol abuse. Conclusions: For intoxications by AHH, effective therapy approaches including forced hyperventilation to increase toxin removal via the lungs are available and require prompt initiation.
Keywords: 1,2-dichloroethane; Aliphatic halogenated hydrocarbons; Carbon tetrachloride; Chloroform; Dichloromethane.
Conflict of interest statement
The author has no conflict of interests related to this publication.
Figures
References
-
- Zimmerman HJ. Hepatotoxicity. Philadelphia: Lippincott Williams & Wilkins; 1999.
-
- Helmenstine AM. Aliphatic hydrocarbon definition. Available from: https://www.thoughtco.com/definition-of-aliphatic-hydrocarbon-604763 .
LinkOut - more resources
Full Text Sources
Miscellaneous