

Possible Post-Traumatic Focal Dystonia Associated with Tau Pathology Localized to Putamen-Globus Pallidus
- PMID: 30637269
- PMCID: PMC6207110
- DOI: 10.1002/mdc3.12626
Possible Post-Traumatic Focal Dystonia Associated with Tau Pathology Localized to Putamen-Globus Pallidus
Abstract
Background: Dystonia is often associated with damage to basal ganglia (BG), but neuropathological assessments of these cases are infrequent.
Methods: A brain was assessed with possible post-traumatic focal dystonia that appeared after an accident occurred during childhood.
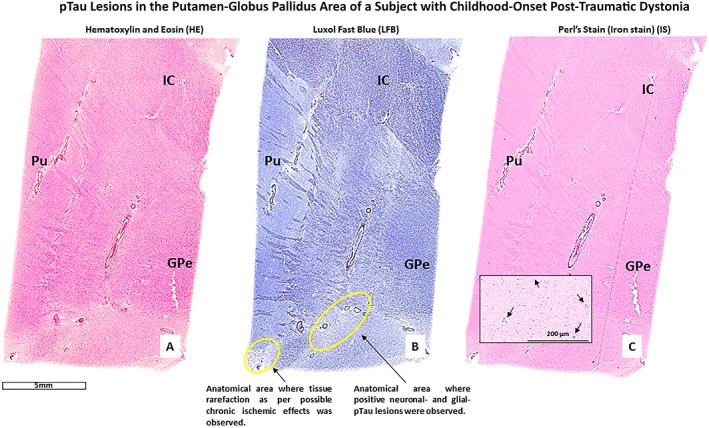
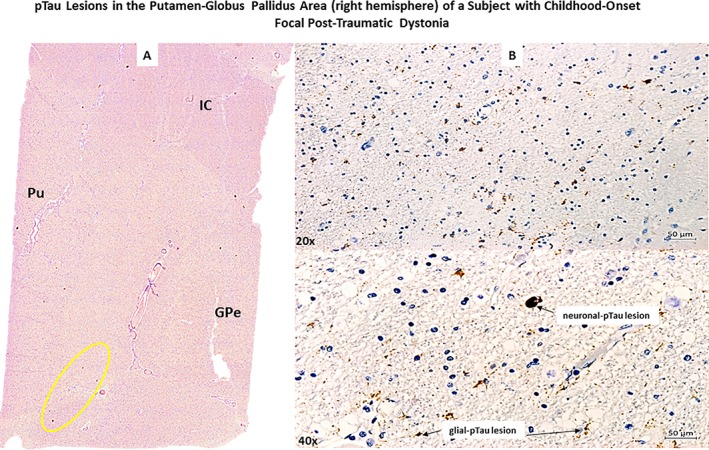
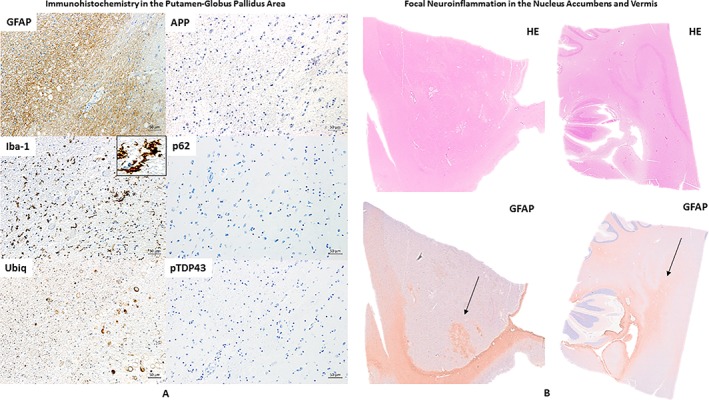
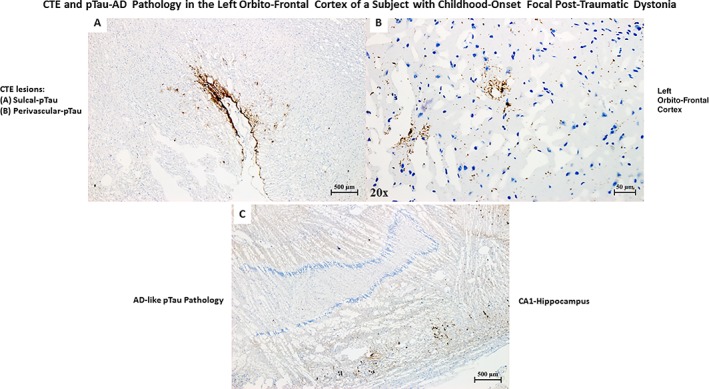
Results: Tau pathology was found within putamen and globus pallidus of the right hemisphere, and chronic traumatic encephalopathy (CTE) was observed in the cortex of the left hemisphere. No diffuse axonal injury (DAI), β-amyloid, ubiquitin, p62, or pTDP43 pathology was found.
Conclusions: Post-traumatic dystonia could be associated with post-traumatic tau pathology formation. However, more cases are necessary to establish causality. The tau lesions found in the BG of this patient did not fit within CTE criteria. We hypothesize that due to the anatomo-histological characteristics of the BG, tau pathology associated with brain traumas produce histopathological patterns different from sulcal-tau pathology, which is the only tau pathology distribution currently accepted as pathognomonic of CTE.
Keywords: CTE spectrum; basal ganglia; post‐traumatic dystonia; tau pathology; traumatic brain injury.
Figures
References
-
- Defazio G, Abbruzzese G, Livrea P, Berardelli A. Epidemiology of primary dystonia. Lancet Neurol. 2004;3:673–678. - PubMed
-
- Steeves TD, Day L, Dykeman J, Jette N, Pringsheim T. The prevalence of primary dystonia: a systematic review and meta‐analysis. Mov Disord. 2012;27:1789–1796. - PubMed
-
- Lohmann K, Klein C. Update on the Genetics of Dystonia. Curr Neurol Neurosci Rep. 2017;17:26. - PubMed
-
- Koller WC, Wong GF, Lang A. Posttraumatic movement disorders: a review. Mov Disord. 1989;4:20–36. - PubMed
-
- Jankovic J. Post‐traumatic movement disorders: central and peripheral mechanisms. Neurology. 1994;44:2006–2014. - PubMed
LinkOut - more resources
Full Text Sources
