

MRI of a painful carpal boss: variations at the extensor carpi radialis brevis insertion and imaging findings in regional traumatic and overuse injuries
- PMID: 30637474
- PMCID: PMC6525668
- DOI: 10.1007/s00256-018-3136-9
MRI of a painful carpal boss: variations at the extensor carpi radialis brevis insertion and imaging findings in regional traumatic and overuse injuries
Abstract
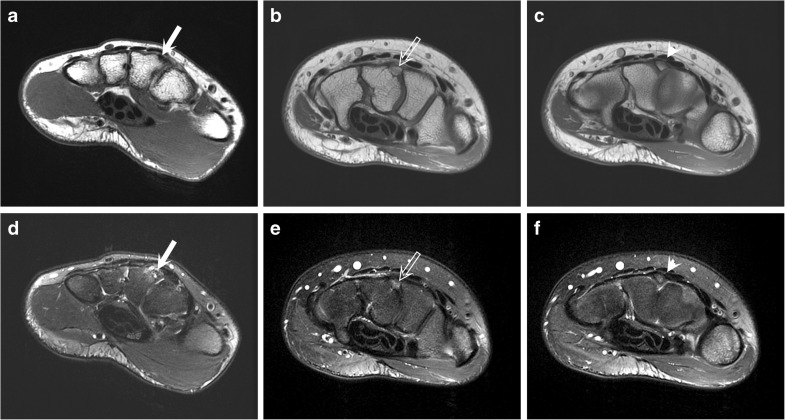
Objective: To report patterns of MRI findings involving carpal boss and extensor carpi radialis brevis (ECRB) tendon insertion in individuals with overuse-related or post-traumatic wrist pain.
Materials and methods: Eighty-four MRI cases with carpal bossing between December 2006 and June 2015 were analyzed by two fellowship-trained musculoskeletal radiologists. The following MRI findings were reviewed: type of carpal bossing (bony prominence, partial coalition, os styloideum), insertion of ECRB tendon (to the 3rd metacarpal, to carpal boss or to both), bone marrow edema (BME), insertion site, and tenosynovitis/tendinosis of ECRB tendon. Clinical information on wrist pain was available on 68 patients.
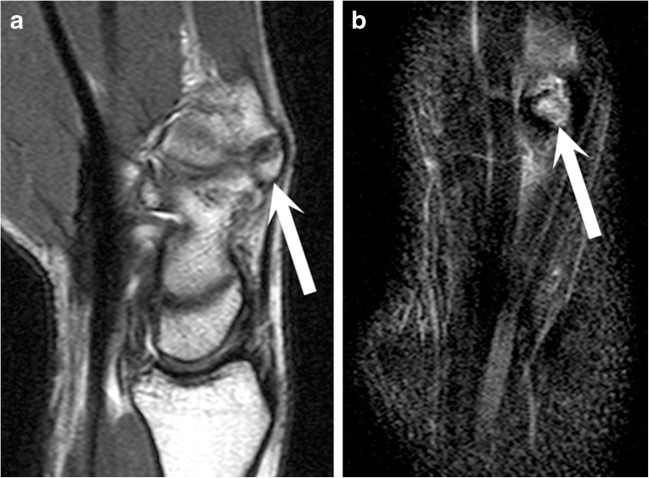
Results: Fused carpal bossing was detected in 21%, partial coalition in 35%, and os styloideum in 44% of the cases. Regional BME was observed in 64% of the cases. When BME specifically at the carpal boss was assessed, 78% of stable and 50% of unstable bosses showed BME (p = 0.035). ECRB tendon inserted on a carpal boss in 20%, on the 3rd metacarpal bone in 35%, and on both sites in 45% of the cases. As BME at the carpal boss was assessed, BME was detected at the respective insertion sites in 71%, 35%, and 66% of the cases (p = 0.015). Dorsal wrist pain was associated with BME as 75% of the patients had regional BME in the vicinity of the carpal boss (p = 0.006).
Conclusion: A spectrum ranging from complete fusion of a boss to an entirely unfused os styloideum exists with a variable ECRB insertional anatomy. BME at the carpal boss is a consistent MRI finding.
Keywords: Bone marrow edema; Carpal boss; Extensor carpi radialis brevis; Magnetic resonance imaging; Os styloideum.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Bassoe E, Bassoe HH. The styloid bone and carpe bossu disease. Am J Roentgenol Radium Ther Nucl Med. 1955;74(5):886–888. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
