

Long-term Survival in Head and Neck Cancer: Impact of Site, Stage, Smoking, and Human Papillomavirus Status
- PMID: 30637762
- PMCID: PMC6907689
- DOI: 10.1002/lary.27807
Long-term Survival in Head and Neck Cancer: Impact of Site, Stage, Smoking, and Human Papillomavirus Status
Abstract
Objectives/hypothesis: Literature examining long-term survival in head and neck squamous cell carcinoma (HNSCC) with human papillomavirus (HPV) status is lacking. We compare 10-year overall survival (OS) rates for cases to population-based controls.
Study design: Prospective cohort study.
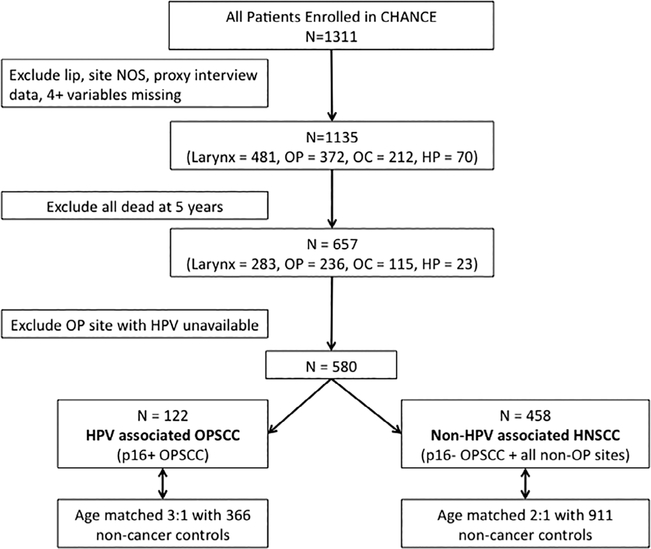
Methods: Cases surviving 5 years postdiagnosis were identified from the Carolina Head and Neck Cancer Study. We examined 10-year survival by site, stage, p16, and treatment using Kaplan-Meier and Cox proportional hazard models. Cases were compared to age-matched, noncancer controls with stratification by p16 and smoking status.
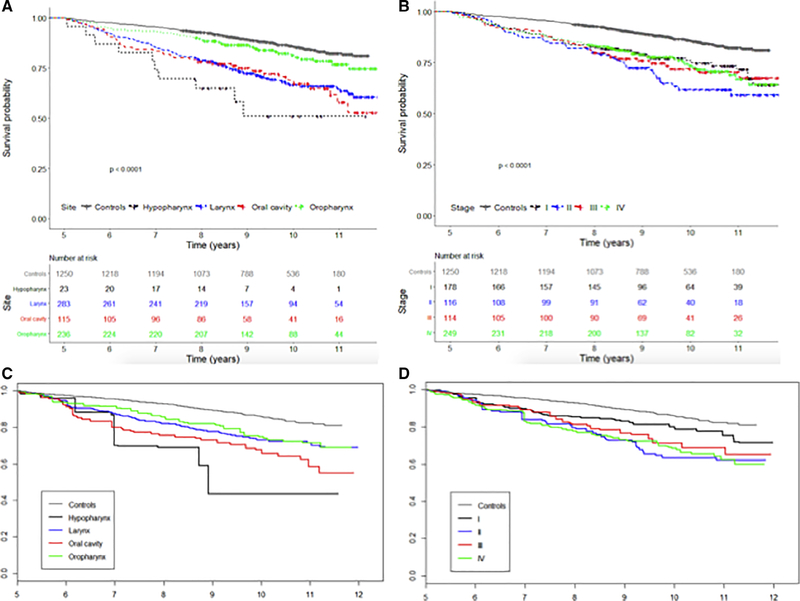
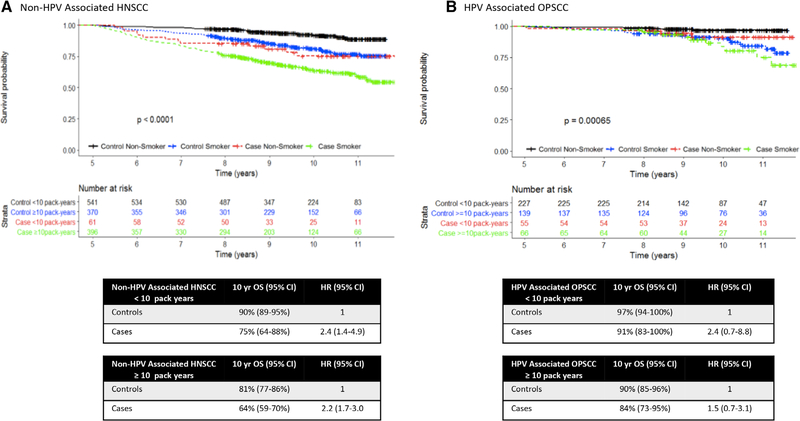
Results: Ten-year OS for HNSCC is less than controls. In 581 cases, OS differed between sites with p16+ oropharynx having the most favorable prognosis (87%), followed by oral cavity (69%), larynx (67%), p16- oropharynx (56%), and hypopharynx (51%). Initial stage, but not treatment, also impacted OS. When compared to controls matched on smoking status, the hazard ratio (HR) for death in p16+ oropharynx cases was 1.5 (95% confidence interval [CI]: 0.7-3.1) for smokers and 2.4 (95% CI: 0.7-8.8) for nonsmokers. Similarly, HR for death in non-HPV-associated HNSCC was 2.2 (95% CI: 1.7-3.0) for smokers and 2.4 (95% CI: 1.4-4.9) for nonsmokers.
Conclusions: OS for HNSCC cases continues to decrease 5 years posttreatment, even after stratification by p16 and smoking status. Site, stage, smoking, and p16 status are significant factors. These data provide important prognostic information for HNSCC.
Level of evidence: 2 Laryngoscope, 129:2506-2513, 2019.
Keywords: Head and neck neoplasms; human papillomavirus; oropharynx; smoking; survival.
© 2019 The American Laryngological, Rhinological and Otological Society, Inc.
Conflict of interest statement
The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Figures
References
-
- Fitzmaurice C, Allen C, Barber RM, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol 2017;3:524–548. - PMC - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017;67:7–30. - PubMed
-
- Hoffman HT, Karnell LH, Funk GF, Robinson RA, Menck HR. The National Cancer Data Base report on cancer of the head and neck. Arch Otolaryngol Head Neck Surg 1998;124:951–962. - PubMed
-
- Boysen M, Natvig K, Winther FO, Tausjo J. Value of routine follow-up in patients treated for squamous cell carcinoma of the head and neck. J Otolaryngol 1985;14:211–214. - PubMed
-
- Blot WJ, McLaughlin JK, Winn DM, et al. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res 1988;48:3282–3287. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
