

The evolution of body composition in oncology-epidemiology, clinical trials, and the future of patient care: facts and numbers
- PMID: 30637983
- PMCID: PMC6351674
- DOI: 10.1002/jcsm.12379
The evolution of body composition in oncology-epidemiology, clinical trials, and the future of patient care: facts and numbers
Abstract
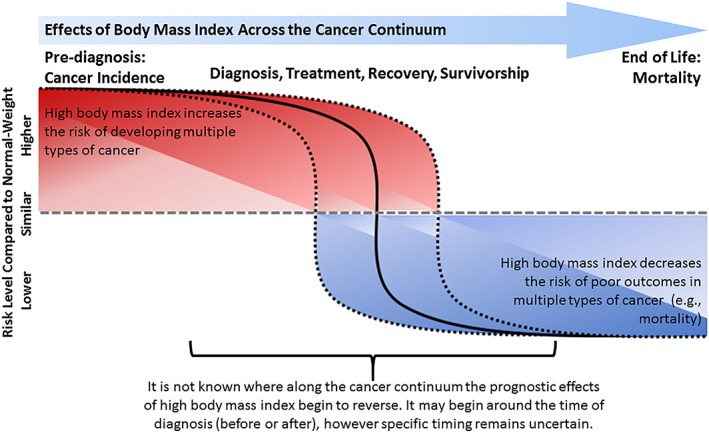
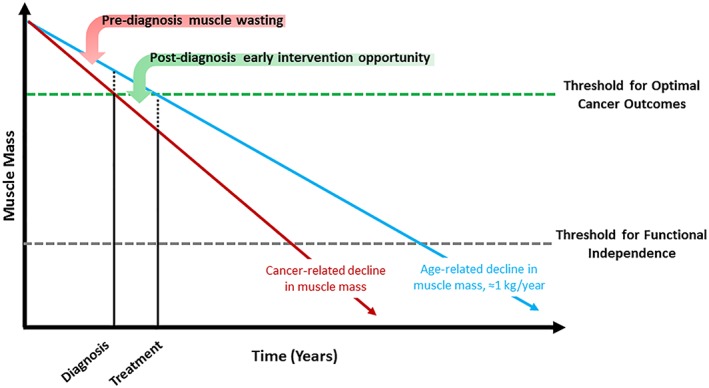
There is growing interest from the oncology community to understand how body composition measures can be used to improve the delivery of clinical care for the 18.1 million individuals diagnosed with cancer annually. Methods that distinguish muscle from subcutaneous and visceral adipose tissue, such as computed tomography (CT), may offer new insights of important risk factors and improved prognostication of outcomes over alternative measures such as body mass index. In a meta-analysis of 38 studies, low muscle area assessed from clinically acquired CT was observed in 27.7% of patients with cancer and associated with poorer overall survival [hazard ratio: 1.44, 95% CI: 1.32-1.56]. Therapeutic interventions such as lifestyle and pharmacotherapy that modify all aspects of body composition and reduce the incidence of poor clinical outcomes are needed in patients with cancer. In a meta-analysis of six randomized trials, resistance training exercise increased lean body mass assessed from dual-energy X-ray absorptiometry [mean difference (MD): +1.07 kg, 95% CI: 0.76-1.37; P < 0.001] and walking distance [MD: +143 m, 95% CI: 70-216; P < 0.001] compared with usual care control in patients with non-metastatic cancer. In a meta-analysis of five randomized trials, anamorelin (a ghrelin agonist) significantly increased lean body mass [MD: +1.10 kg, 95% CI: 0.35-1.85; P = 0.004] but did not improve handgrip strength [MD: 0.52 kg, 95% CI: -0.09-1.13; P = 0.09] or overall survival compared with placebo [HR: 0.99, 95% CI: 0.85-1.14; P = 0.84] in patients with advanced or metastatic cancer. Early screening to identify individuals with occult muscle loss, combined with multimodal interventions that include lifestyle therapy with resistance exercise training and dietary supplementation combined with pharmacotherapy, may be necessary to provide a sufficient stimulus to prevent or slow the cascade of tissue wasting. Rapid, cost-efficient, and feasible methods to quantify muscle and adipose tissue distribution are needed if body composition assessment is to be integrated into large-scale clinical workflows. Fully automated analysis of body composition from clinically acquired imaging is one example. The study of body composition is one of the most provocative areas in oncology that offers tremendous promise to help patients with cancer live longer and healthier lives.
Keywords: Cancer; Cohort study; Computed tomography; Metabolism; Obesity paradox; Randomized trial.
© 2019 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of the Society on Sarcopenia, Cachexia and Wasting Disorders.
Figures
References
-
- Martin L, Watanabe S, Fainsinger R, Lau F, Ghosh S, Quan H et al. Prognostic factors in patients with advanced cancer: use of the patient‐generated subjective global assessment in survival prediction. J Clin Oncol 2010;28:4376–4383. - PubMed
-
- Hopkins JJ. Sawyer MB. A review of body composition and pharmacokinetics in oncology. Expert Rev Clin Pharmacol 2017;10:947–956. - PubMed
-
- Shachar SS, Williams GR, Muss HB, Nishijima TF. Prognostic value of sarcopenia in adults with solid tumours: a meta‐analysis and systematic review. Eur J Cancer 2016;57:58–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
