

The depth of the implant mucosal tunnel modifies the development and resolution of experimental peri-implant mucositis: A case-control study
- PMID: 30638273
- PMCID: PMC6593437
- DOI: 10.1111/jcpe.13066
The depth of the implant mucosal tunnel modifies the development and resolution of experimental peri-implant mucositis: A case-control study
Abstract
Background: Resolution and prevention of peri-implant mucositis are a key in preventing peri-implantitis. This case-control study aims to assess the modifying effect of a deep mucosal tunnel (DMT) on the induction and resolution phases of experimental peri-implant mucositis.
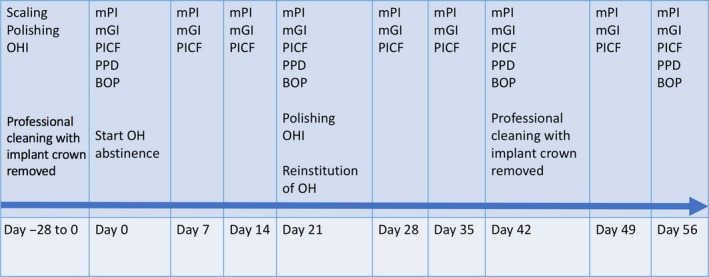
Methods: Nineteen subjects with a tissue level implant were assigned to cases (DMT, depth ≥3 mm) or controls (shallow mucosal tunnel ≤1 mm, SMT). Subjects underwent a standard experimental peri-implant mucositis protocol characterized by an oral hygiene optimization phase, a 3-week induction phase using an acrylic stent to prevent self-performed oral hygiene at the experimental implant, and a 3 + 2 weeks resolution phase. Modified plaque (mPI), gingival index (mGI) and peri-implant sulcus fluid IL-1β concentrations were measured over time. Differences between DMT and SMT were assessed with the Mann-Whitney test.
Results: Modified plaque index and mGI increased in parallel during the induction phase. After resumption of oral hygiene practice, mPI and mGI resolved towards baseline values in the SMT group. In DMT, mPI and mGI values diverged: plaque resolved but resolution of inflammation was delayed and of smaller magnitude during the first 3 weeks after resumption of oral hygiene. IL-1β concentrations were significantly higher in DMT at 21 days (end of induction) and during the resolution phase corroborating the clinical findings. Removal of the crown and submucosal professional cleaning were needed to revert mGI to baseline values in DMT implants.
Conclusions: The depth of the mucosal tunnel modifies the resolution of experimental peri-implant mucositis at transmucosal implants. This observation raises important questions on the effectiveness of self-performed oral hygiene in cases where implants are placed deeper and the ability to resolve mucositis and effectively prevent peri-implantitis in such situations.
Keywords: case-control study; dental implant; experimental gingivitis; mucositis prevention; peri-implant mucositis; peri-implantitis prevention; transmucosal implant.
© 2019 The Authors. Journal of Clinical Periodontology Published by John Wiley & Sons Ltd.
Conflict of interest statement
Authors report no conflict of interest related to this study.
Figures




References
-
- Berglundh, T. , Armitage, G. , Araujo, M. G. , Avila‐Ortiz, G. , Blanco, J. , Camargo, P. M. , … Zitzmann, N. (2018). Peri‐implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions. Journal of Clinical Periodontology, 45(Suppl 20), S286–S291. 10.1111/jcpe.12957 - DOI - PubMed
-
- Chappuis, V. , Bornstein, M. M. , Buser, D. , & Belser, U. (2016). Influence of implant neck design on facial bone crest dimensions in the esthetic zone analyzed by cone beam CT: A comparative study with a 5‐to‐9‐year follow‐up. Clinical Oral Implants Research, 27, 1055–1064. 10.1111/clr.12692 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
