

Mortality in US veterans with pulmonary hypertension: a retrospective analysis of survival by subtype and baseline factors
- PMID: 30638433
- PMCID: PMC6381440
- DOI: 10.1177/2045894019825763
Mortality in US veterans with pulmonary hypertension: a retrospective analysis of survival by subtype and baseline factors
Abstract
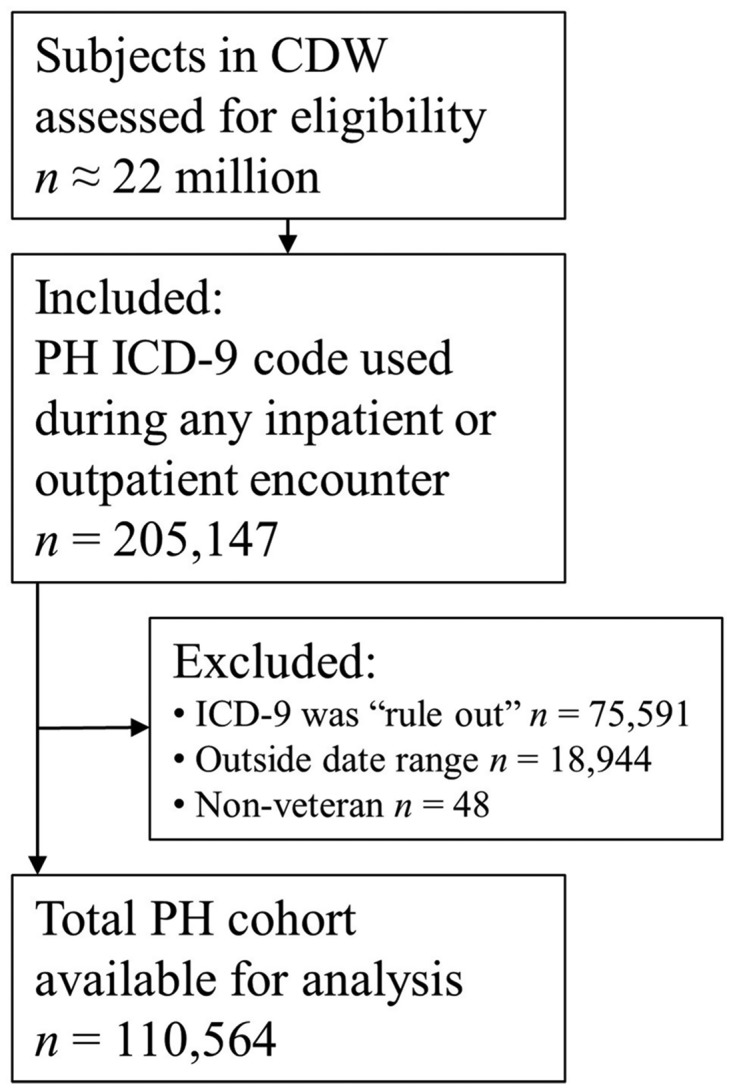
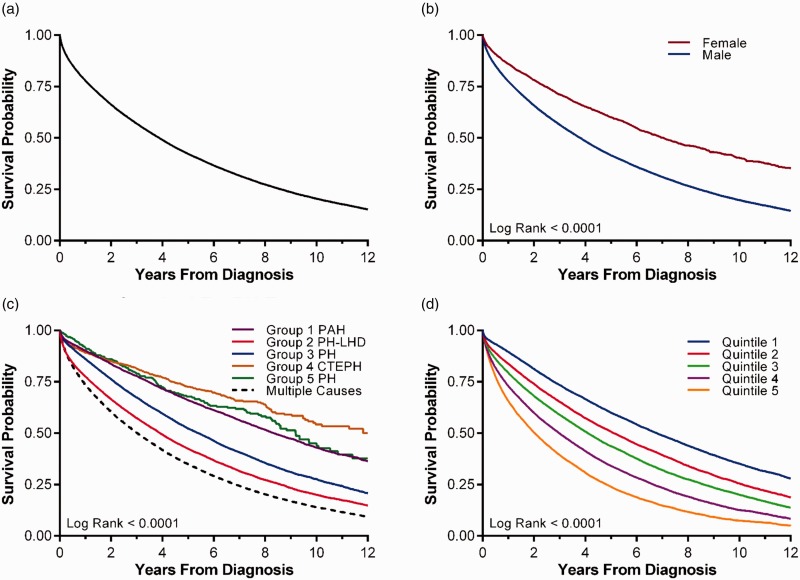
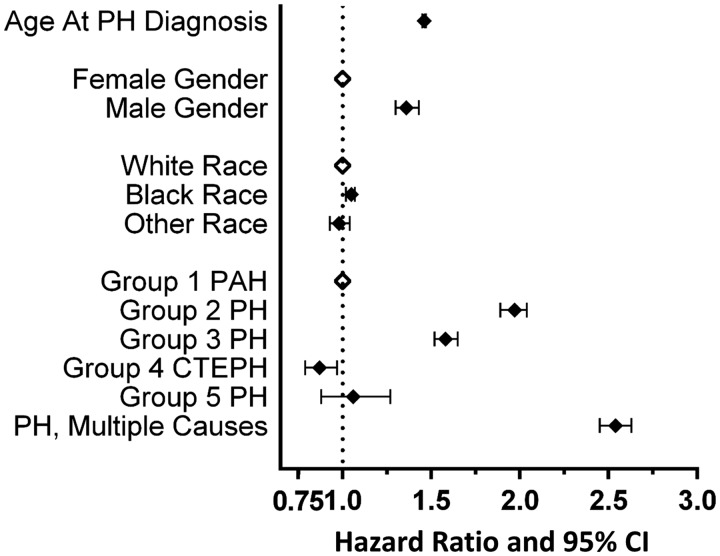
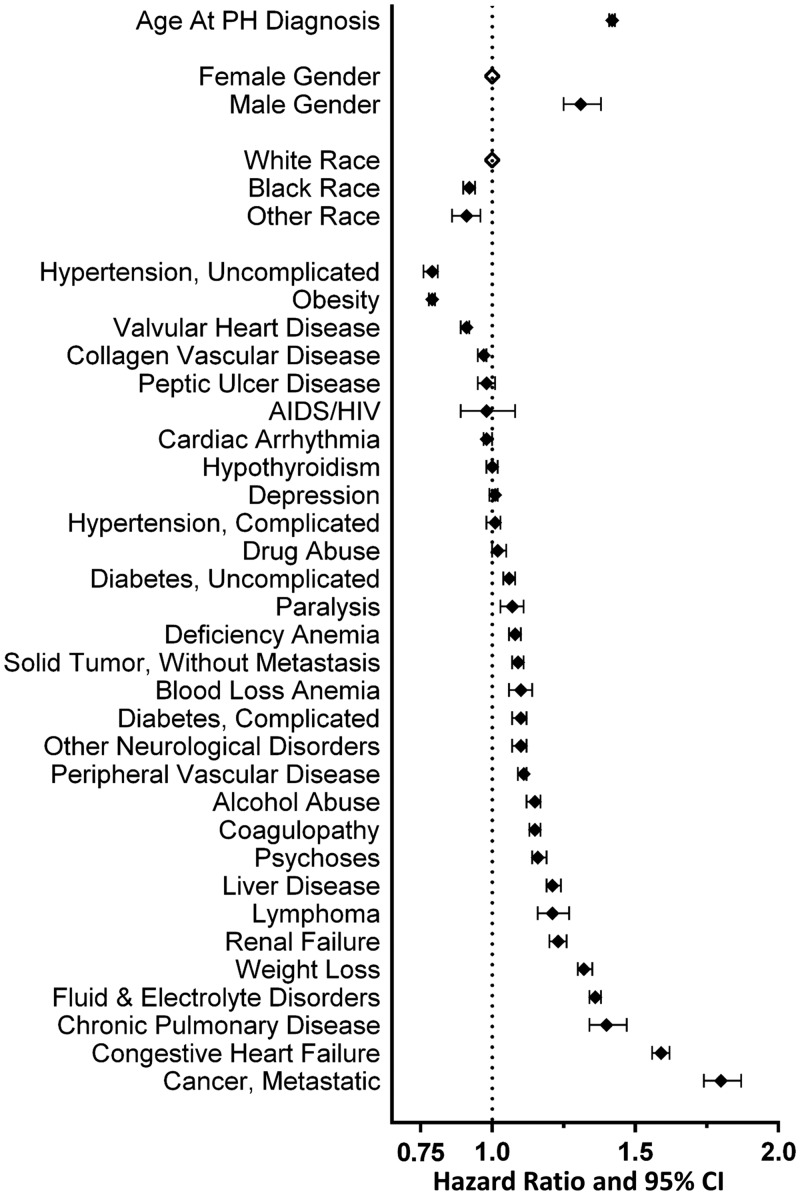
Pulmonary hypertension (PH) occurs when the pulmonary vasculature is itself diseased or becomes affected secondarily by comorbid conditions, commonly left heart or lung disease. The high prevalence of chronic cardiopulmonary conditions among patients served by Veterans Health Administration (VHA) suggests this population may be particularly susceptible to PH. We sought to identify clinical features and outcomes in veterans diagnosed with PH. We utilized the VHA Corporate Data Warehouse to identify veterans diagnosed between January 1, 2003 and September 30, 2015, assess relevant patient characteristics and their survival time. The effects of PH subtype and baseline factors on outcome were estimated by Cox modeling. There were 110,564 veterans diagnosed with PH during the study period. These veterans were predominantly male, had median age 70.2, and had a high burden of comorbid conditions. PH was frequently due to left heart and/or lung disease. Average survival after PH diagnosis was 3.88 years. Compared with other types, PH due to left heart disease, lung disease or both had shorter survival. This large retrospective study of veterans demonstrates the significance of PH due to left heart and/or lung disease which was common and had high risk of death. Multi-comorbidity was common and added to risk. These findings underscore the need for risk assessment tools for subjects with non-Group 1 PH and novel management strategies to improve their outcome. This study details the largest retrospective cohort assembled for evaluation of secondary PH and allows hypothesis-generating inquiries into these common conditions that are rarely prospectively studied.
Keywords: comorbidity; pulmonary hypertension; retrospective cohort study; risk factors; survival.
Figures
References
-
- Galiè N, Humbert M, Vachiery J-L, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016; 37: 67–119. - PubMed
-
- McGoon MD, Benza RL, Escribano-Subias P, et al. Pulmonary arterial hypertension: Epidemiology and registries. J Am Coll Cardiol 2013; 62: D51–D59. - PubMed
-
- Hoeper MM, Bogaard HJ, Condliffe R, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol 2013; 62: D42–D50. - PubMed
-
- Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med 1987; 107: 216–223. - PubMed
-
- Gall H, Felix JF, Schneck FK, et al. The Giessen Pulmonary Hypertension Registry: Survival in pulmonary hypertension subgroups. J Heart Lung Transplant 2017; 36: 957–967. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
