

Report from the National Institute of Allergy and Infectious Diseases workshop on "Atopic dermatitis and the atopic march: Mechanisms and interventions"
- PMID: 30639346
- PMCID: PMC6905466
- DOI: 10.1016/j.jaci.2019.01.003
Report from the National Institute of Allergy and Infectious Diseases workshop on "Atopic dermatitis and the atopic march: Mechanisms and interventions"
Abstract
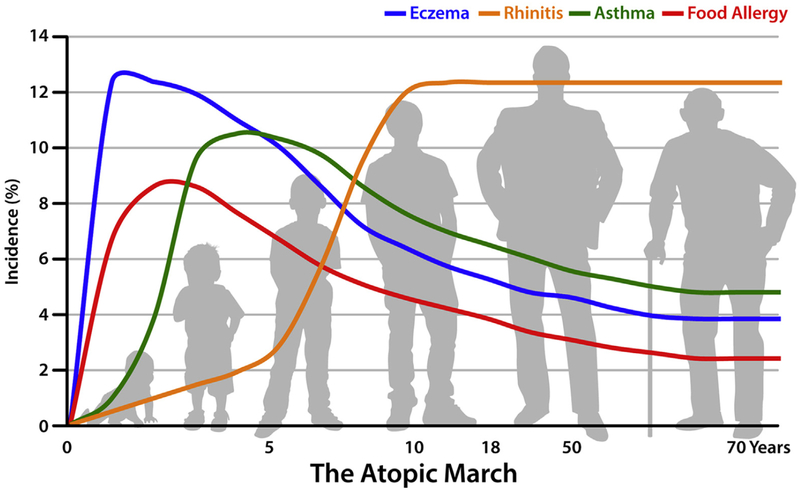
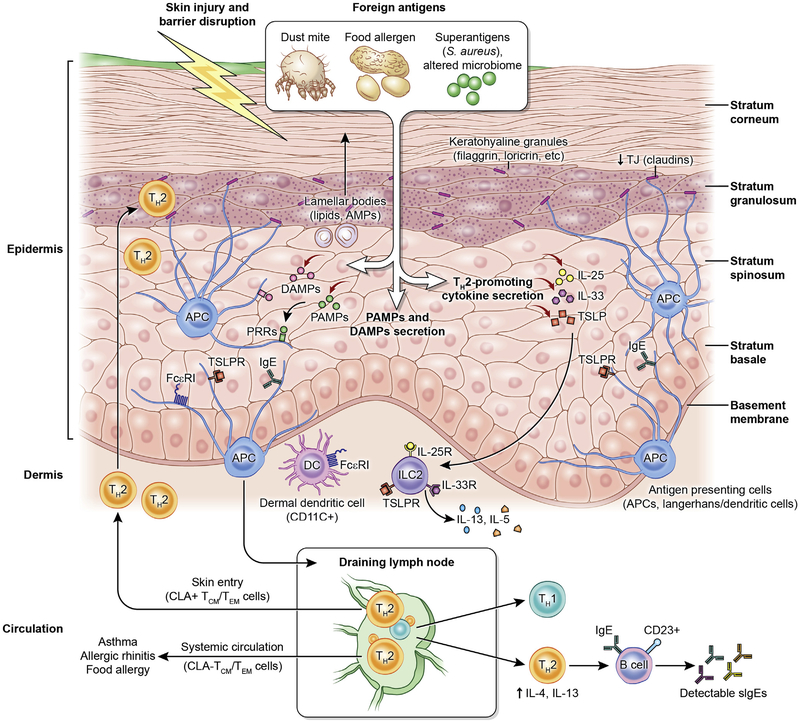
Atopic dermatitis (AD) affects up to 20% of children worldwide and is an increasing public health problem, particularly in developed countries. Although AD in infants and young children can resolve, there is a well-recognized increased risk of sequential progression from AD to other atopic diseases, including food allergy (FA), allergic rhinitis, allergic asthma, and allergic rhinoconjunctivitis, a process referred to as the atopic march. The mechanisms underlying the development of AD and subsequent progression to other atopic comorbidities, particularly FA, are incompletely understood and the subject of intense investigation. Other major research objectives are the development of effective strategies to prevent AD and FA, as well as therapeutic interventions to inhibit the atopic march. In 2017, the Division of Allergy, Immunology, and Transplantation of the National Institute of Allergy and Infectious Diseases sponsored a workshop to discuss current understanding and important advances in these research areas and to identify gaps in knowledge and future research directions. International and national experts in the field were joined by representatives from several National Institutes of Health institutes. Summaries of workshop presentations, key conclusions, and recommendations are presented herein.
Keywords: Atopic march; asthma; atopic dermatitis; biomarkers; food allergy; interventions; skin barrier; skin microbiome.
Copyright © 2019 American Academy of Allergy, Asthma & Immunology. All rights reserved.
Conflict of interest statement
Disclosure of potential conflict of interest: D. Y. M. Leung has received personal fees from Regeneron Pharmaceuticals and Sanofi-Genzyme Pharmaceuticals and has received grants from MedImmune Pharmaceuticals, Pfizer Pharmaceuticals, and Incyte Corporation. L. A. Beck has received grants from Abbvie, Realm Therapeutics, Regeneron, and Pfizer; has received personal fees from Abbvie, Astra-Zeneca, Allakos, Boehringer Ingelheim, Celgene, Eli Lilly, GlaxoSmithKline, Leo Pharma, Novan, Novartis, Realm Therapeutics, Regeneron, and Sanofi; and has received stock from Pfizer and Medtronics. W. W. Busse has received personal fees from 3M, Boehringer Ingelheim, Boston Scientific, AstraZeneca, GlaxoSmithKline, Novartis, Sanofi/Genzyme, Teva, Genentech, Elsevier, Medscape, ICON Clinical Research, Regeneron, and PrEPBiopharm. T. A. Chatila is a member of the Scientific Advisory Board for Consortia Therapeutics, has received a grant from the National Institutes of Health (NIH; 5 R01 AI126915), and has a patent pending for Therapeutic microbiota for the treatment and/or prevention of food allergy (US20180117098A1). J. E. Gern has received a grant from the NIH/National Institute of Allergy and Infectious Diseases (NIAID); has received personal fees from PREP Biopharm, Regeneron, and MedImmune; has received stock from Melissa Vaccines; and has patents pending for Methods of Propagating Rhinovirus C in Previously Unsusceptible Cell Lines and Adapted Rhinovirus C. E. Guttman-Yassky has received grants and personal fees from Dermavant, DS Biopharma, Galderma, Glenmark, LEO Pharmaceuticals, Novartis, Pfizer, Regeneron Pharmaceuticals, and Union Therapeutics; has received grants from Dermira, Innovaderm, Novan, Ralexar, and Janssen Biotech; and has received personal fees from Eli Lilly, Escalier, Kyowa Kirin, Mitsubishi Tanabe, Sanofi, DBV, EMD Serono, and Flx Bio. A. D. Irvine has received personal fees from Sanofi/Regeneron. B. S. Kim has received grants from the NIH, the Doris Duke Charitable Foundation, LEO Pharma, and Celgene; has received personal fees from Abb-Vie, Concert, Celgene, Kiniksa, Menlo, Pfizer, Regeneron, Sanofi, Theravance, Incyte, and Nuogen Pharma; has a patent pending (US Provisional Application no. 62/295,875); and owns personal stock in Gilead and Mallinckrodt. G. Lack reports grants from the NIAID/NIH) and the UK Food Standards Agency (FSA); other support from Food Allergy Research & Education (FARE), MRC & Asthma UK Centre, the UK Department of Health through NIHR, the National Peanut Board (NPB), and Osem during the conduct of the study; and other support from DBV Technologies and Mighty Mission Me outside the submitted work. K. C. Nadeau reports grants from NIAID; other support from Novartis, personal fees from Regeneron; grants from FARE and EAT; and other support from Sanofi, Astellas, Nestle, BeforeBrands, Alladapt, ForTra, Genentech, AImmune Therapeutics, and other from DBV Technologies outside the submitted work. E. L. Simpson has received a grant from the NIH/National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS; U34 AR065739–02) and Regeneron Pharmaceuticals and has received personal fees from Regeneron Pharmaceuticals. J. M. Spergel reports grants and personal fees from DBV Technologies and Regeneron; grants and other support from the NIH; personal fees from FARE, the American Partnership for Eosinophilic Disorders, Pfizer, Kaleo, and GlaxoSmithKline; and grants from Aimmune Therapeutics. R. A. Wood reports grants from NIAID, Astellas, Sanofi, DBV, Regeneron, and HAL Allergy and royalties from UpToDate. J. A. Woodfolk reports grants from the NIH/NIAID and the NIH/NIAMS and personal fees from Boehringher Ingelheim. S. F. Ziegler has received a grant from the NIH. The rest of the authors declare that they have no relevant conflicts of interest.
Figures
References
-
- Bieber T Atopic dermatitis. N Engl J Med 2008;358:1483–94. - PubMed
-
- Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI. ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol 2009;124: 1251–8.e23. - PubMed
-
- Wahn U What drives the allergic march? Allergy 2000;55:591–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
